Today I cannot receive one of the most common and beneficial oral health activities, a six-month dental visit with my dental provider, Kaiser Permanente.
Healthy smile, photo by Rudy Owens
The reason why? I am refusing to have a panoramic X-ray.
This potentially profitable medical procedure for some dental practices is a recent development in the oral health field that has followed the proliferation of the panoramic technology in the past several decades. However, these are not universally recognized in developed nations as a best health practice for routine dental care compared to bitewing X-rays, which my past dentists used. Neither is without risk. … [More of my guest column in the Sept. 16, 2015, Lund Report health newsletter can be found here.]
UPDATE Sept. 20, 2015: One critic of my column printed on the Lund Report web site wrote this statement, apparently to correct the record about what the American Dental Association’s guidelines are:
The ADA’s guidelines from 2012 actually state that for new patients (such as Mr. Owen) a panoramic radiographic exam is recommended so it seems that Kaiser is following the ADA’s recommendation.
“Individualized radiographic exam consisting of Individualized evaluated for dental radiographic exam radiographic exam posterior bitewings with panoramic exam or radiographic exam, diseases and dental consisting of consisting of posterior bitewings and selected periapical based on clinical development selected periapical/ posterior bitewings images. A full mouth intraoral radiographic signs and occlusal views and/ with panoramic exam is preferred when the patient has symptoms. or posterior exam or posterior clinical evidence of generalized dental disease bitewings if bitewings and or a history of extensive dental treatment.”
I found this comment remarkable because the author of it, someone who identified him/herself as Peta Pita (likely an assumed name, and this person misspelled my name too), did not mention the statement that immediately precedes guidelines for all radiography recommendations for people of all ages. So this comment is factually inaccurate.
The ADA foremost states [I put in bold for emphasis]: “These recommendations are subject to clinical judgment and may not apply to every patient. They are to be used by dentists only after reviewing the patient’s health history and completing a clinical examination. Even though radiation exposure from dental radiographs is low, once a decision to obtain radiographs is made it is the dentist’s responsibility to follow the ALARA Principle (As Low as Reasonably Achievable) to minimize the patient’s exposure.”
What’s more, the ADA also states for adult patients the following (and this does not include panoramic radiography): “Adult dentate patients, who receive regularly scheduled professional care and are free of signs and symptoms of oral disease, are at a low risk for dental caries. Nevertheless, consideration should be given to the fact that caries risk can vary over time as risk factors change. Advancing age and changes in diet, medical history and periodontal status may increase the risk for dental caries. Therefore, a radiographic examination consisting of posterior bitewings is recommended at intervals of 24 to 36 months.”
I enclose a screen snapshot for those who may be unsure how to intepret a recommendation table. This section covers the issue mentioned above, just including recommendations for adults:
Note the statement on top of the table the is the overarching guideline any dental practitioner may wish to follow, if they choose to follow the ADA’s recommendations. Note, the ADA does not represent how all countries and other international organizations who promote oral health set guidelines for dental radiography. Remember, the U.S. health care system is the least efficient and most costly in the world, and a wealth of data highlight the over-use of unecessary medical tests as a major factor leading to this problem. Here is just one example of that: http://www.commonwealthfund.org/publications/fund-reports/2014/jun/mirror-mirror.
The River Rouge neighbhorhood is lined with broken and burned homes, like these.
As a native of Detroit, I present this first of several essays, with a profound sense of sadness. (See my photo blog for my first photo essay.)
Here’s the proof if you need it–Michigan verifies I am a native Detroiter.
It is hard to accept that my birthplace, this once great global city, has become a symbol for American industrial decay and capitalism’s larger ills. At one point, Detroit boasted nearly 2 million residents in the 1950s. Today is barely counts 700,000 residents. [Updated census figures, 5/5/2015.]
In its heyday of bustling industrial production, Detroit served as a global icon for American ingenuity, industrial might, and economic power. During World War II, when the larger metro area produced the country’s war weaponry to defeat the Axis powers, Detroiters proudly called their city the Arsenal of Democracy. In the 1920s and 1930, about 40 percent of all automobiles were manufactured in the Motor City and the Ford River Rouge plant was the world’s largest.
Today, Detroit is known more as the murder capital of the United States, and the arson capital. All told, 90,000 fires were reported in 2008, double New York’s number—for a city 11 times larger—according to Mark Binelli, author of Detroit City is the Place to Be. It is the epitome of racial politics. Binelli notes, 90,000 buildings are abandoned, and huge swaths of the 140-square mile urban area are now returning to nature. Beavers, coyotes, deer, packs of wild dogs, and foxes are now reported in the city.
Photo Courtesy of Detroit Dog Rescue: up to 50,000 wild dogs roam Detroit.
I just visited Detroit, and the trip had a more profound impact on me than I was prepared for. How is it that our country could undertake two overseas wars to conquer and rebuild nations—Iraq and Afghanistan—and yet abandon a city that helped to make the country the global power it once was.
National partisan politics have played a role, with Detroit becoming a symbol of the Democratic Party’s failure, as a black city and union city, in the eyes of white and conservative detractors. Then there are NAFTA (pushed by Bill Clinton) and industry fleeing the country for cheaper manufacturing from global suppliers and gross mismanagement of the Big 3 automobile companies, two of whom were bailed out by U.S. taxpayers in 2009.
White flight eventually followed long-simmering racial tensions. There have been Detroit race riots in 1863, 1943, 1967, and 1987. Those riots were stoked by historic racism, redlining, job discrimination, and the building of freeways that helped to destroy America’s inner cities. Today, some criminal fringe actors among Detroit’s mostly black residents are burning what’s left of their own city, for at times just the hell of it.
A burned and destroyed home is a common site. This one is near Livernois and I-75.
Charlie LeDuff, author of Detroit, An American Autopsy, painted a heart-breaking tale of the city’s self-destructive conflagrations through the tales of firemen trying to combat the arsonists. “In this town, arson is off the hook,” said a firefighter to LeDuff. “Thousands of them a year bro. In Detroit, it’s so fucking poor that a fire is cheaper than a movie. A can of gas is three-fifty, and a movie is eight bucks, and there aren’t any movie theaters left in Detroit so fuck it.” (I will do a photo essay of fire-ravaged homes shortly.)
That latest malaise, on top of repeated political scandals and corruption by the city’s bureaucrats and criminal politicians, was a crushing bankruptcy filing in the face of an $18 billion debt. In December 2014, after a year an a half in limbo, a grand bargain was struck with creditors, the city, the state, and private industry that prevented the city from selling its city-owned artwork (Rembrandts, Van Goghs, and more) in the world famous Detroit Institute of Arts.
The Diego Rivera Mural at the Detroit Institute of Arts highlights the brutal and still glory days that once were Detroit, the Motor City.
As I wandered the glittering white palace that is the DIA, I wondered, what’s more important, this art or the blocks and blocks of emptied neighborhoods that most of this country has forgotten.
Coming back to Portland was hard. I posted a comment on Twitter as soon as I arrived back home how bizarre it was to be back in the whitest city in North America, Portland, after spending time in the city that America defines as African-American.
This week, I attempted to do what consumers world over try to do: figure out the cost of a transaction to make an informed decision before I acted. Everyone from market shoppers in Malawi to mega-billionaires choosing to invest their capital does this. They all are promoting their self-interest and also trying to save or even make money.
I wanted to know what a doctor’s visit would cost and how much truly might be or might not be covered. If needed, I wanted to know if I had to find a better bargain, if the first option would not be an affordable activity with my plan. It might have been easier to walk across the Sahara barefoot, without water.
What I tried to do is impossible for American consumers trying to figure out the price of just about every medical procedure, doctor’s or dentist’s visit, and hospital activity.
Photo courtesy of Harvard, showing people protesting for health care access. But most of us want health pricing information too, and are prevented from getting that by providers and insurance companies.
Today, except the for very rich who do not need insurance, there is no such thing as a functioning U.S. health care market, where consumers can freely choose to pick their providers and choose lower-cost options. Insurance companies and providers do everything possible to hide prices and bully and even threaten insured consumers who are trying to make choices that occur in rational and functioning markets.
The Commonwealth Fund notes, “… the U.S. health care market is unlike any other market: patients rarely know what they’ll pay for services until they’ve received them; health care providers bill different payers different prices for the same services; and privately insured patients pay more to subsidize the shortfalls left by uninsured patients. What’s more, prices for health services vary significantly among providers, even for common procedures such as laboratory tests or mammograms, although there’s no consistent evidence showing that higher prices are linked to higher quality.”
The Commonwealth Fund argues that even some modest reforms in pricing transparency, with our broken system, could lead consumers to “receive high-quality services from lower-cost providers … This, in turn, could encourage competition among providers based on the value of care—not just on reputation and market share.”
So what does this have to do with me and my experience? Everything, actually.
Gauging consumers one by one: the thousand cuts approach:
For years, I have consistently tried to get dentists and doctors to give me a price quote before a visit. To date, I have never had any medical provider provide me prices or codes without fighting tooth and nail, and often it is with caveats that claim they are exempt from any responsibility if their pricing information is wrong, even with the diagnosis code for a routine checkup.
Here is how the health provider and health insurance fraud and rip-offs work, patient by patient, and this is how it recently happened with me.
Step one: Call the provider and have them evade sharing information.
“We can’t provide you a diagnosis code until you see the physician.” To which I reply, “I am trying to understand if the charge will be covered by my insurance company.” They answer, “We can’t do that because the doctor may do [fill the BS line that you prefer].”
Step two:Call the insurance companyand have them not tell you if a possible charge by a provider is within their “usual and customary charges”—a term that is behind a wall of secrecy and never shared with consumers, ever.
“Hello, I’m trying to determine if my visit to my physician is covered and if the charges are within your accepted ranges.” They reply, “Sir, we can’t do that. We’d need to know the diagnosis codes and procedure codes before we can possibly investigate that.”
To which I reply, “Sir/mam, I don’t have that. Doctors’ offices never tell you that. I don’t have the codes.” Or, if I was able to get a code for a check up, “Here is the diagnosis code [fill in code], what is your accepted charge.”
The reply could be, “Sir, I told you we would need the diagnosis code to investigate…” Me interrupting, “Sir/mam, I just told you they won’t give me that code, and no doctor…” Them interrupting, “Sir, you are becoming agitated, stop interrupting me. I was saying we need the diagnosis….” Me interrupting, “I am not becoming agitated. I am behaving perfectly rationally. I just want to know what this will cost and how it will be covered.”
They reply, “Sir, I have already told you, without a diagnosis code and procedure code, we are not able to provide you…” Me interrupting again, “Sir/mom, did you just hear me when I said the office will not provide me with a diagnosis code.”
Usually such a song and dance can go on for about five or 10 minutes. In the end, the insurance reps will likely have bullied the consumer and employed their standard and tested propaganda that justifies preventing nearly all consumers from knowing if any medical procedure will truly be covered and at what level. The same works for hospitals, clinics, and other practices, who will not share their prices.
In short, they have created a system that perpetuates waste, fraud, and abuse, one patient at a time, systemwide—and it is a system that remains protected by powerful special and political interests who profit from this.
Who the hell created this mess and what it means:
We can thank our political process that encourages special interests to buy influence and bankroll candidates with campaign donations for a good chunk of this mess. We can also thank the so-called health insurance companies from protecting their market share that makes the United States the most inefficient and most expensive health care system among all developed nations.
The Commonwealth Fund in 2014 reported the U.S. trailed other developing nations in health care outcomes and costs.
The Commonwealth Fund also has found that the U.S. system underperforms and has worse outcomes than 10 other industrial nations, mirroring past findings. No surprises there—this fact has been reported by health and public health researchers now for years. The U.S. economy devotes an absurd 17.7 percent of GPD to health care spending, almost double that of its peers.
How the United States compares to its peers in health care spending by GPD. Source: Commonwealth Fund.
The Center for American Progress has described the consolidation of power by the bloated middlemen of our dysfunctional health care system as a crisis, due to consolidation and market control. The center reports the “lack of competition has led to growing insurer profits, increased costs and reduced coverage for enrollees, an epidemic of deceptive and fraudulent conduct, and rapidly escalating costs.”
Theodore Roosevelt in 1912 led one of the earliest efforts to support a national health plan in the United States, and received support from progressives at the National Progressive convention that year.
From the early 1900s to the present, major efforts to reform the U.S. health care system to create a national health system have failed. Some of the principal profiteers that have safeguarded the status quo are the monolithic health insurance companies, like Premera Blue Cross, my provider.
Other bloated health benefits providers include Aetna, Wellpoint, UnitedHealth Group, Cigna MetLife, and Humana. All of these companies are major political players who donate generously to members of Congress and state officials.
The health insurance model is a system vigorously defended by the GOP-controlled Congress, whose members theoretically support open markets, when in fact GOP members have attempted to derail the Affordable Care Act more than 50 times as of January 2015. And that reform was ultimately about reforming the existing health insurance market, not changing the system to promote openness in pricing or improving population health that is linked to universal health care systems.
The ACA only offered modest efforts to promote transparency. The law requires hospitals to publish and annually update a list of standard charges for their services. Other provisions about requiring exchanges to show prices are at best failed and complicated efforts that do nothing to break the wall of secrecy that has fed the beast that is our health insurance market.
The most pathetic part of this is, when I as a consumer try to do something, I am labeled a problem and seen as the bad guy. But I am OK with that, because doing the right thing always will meet with resistance. I have never kissed a doctor’s feet or behind, or those of companies that profit through monopolistic practices. I do not intend to start now. It just rubs me that today when I see the doctor, and tell him to make his pricing transparent, he will roll his eyes and give that “whatever look.”
The resurgence and outbreak of the most contagious virus on the planet, measles, has led to a swarm of media stories that have tried to report responsibly about the pockets of perpetrators of bogus science.
Even in the face of rock-solid research, done at the population level, proving without question that there is no link between autism and autism spectrum disorder and the measles, mumps, and rubella vaccine, the naysayers continue to promote ideas that have the same validity as racial eugenics of scientific quacks and Nazi racists. There are many parties who are helping to fan the flames of ignorance that threaten innocent children who have no ability to tell parent deniers that they put infants at serious health risks when they do not have their kids immunized from extremely infectious and very preventable illnesses.
This photo, courtesy of the BBC, shows a vaccine vial for the commonly used vaccine used to prevent the spread of very contagious viral illnesses.
Former Playmate Jenny McCarthy and clusters of deniers on both sides of the political spectrum are partially responsible for the resurgence of measles we are seeing around the country today.
What is particularly irresponsible is when formerly balanced media outlets choose to fan the debate flames to promote their products when there is no scientific or medical basis for claiming the issue is “a debate” as opposed to a public health crisis that requires layers of interventions to ensure the best health outcomes for all of us.
Tonight, I read the Oregonian newspaper’s story seeking to solicit input from science deniers with this astounding headline: “In the debate over vaccines, where do you stand?” At the bottom of the story were numerous blog comments that were not moderated. No surprise the journalistic adventure gave Portland’s now world-famous anti-fluoride, vaccination-denier, and anti-public-health community another platform to spout nonsense. Such sloppy journalism keeps bogus science alive and well, even when quackery like eugenics is now considered bad and un-modern. (In the end, quack science is still quack science.)
The Oregonian newspaper ran this story in its online edition on Feb. 4, 2015, which helps promote unproven public health skepticism that is thoroughly debunked as junk science.
Reporter Kjerstin Gabrielson wrote, “What influenced your decision to immunize or not immunize your children? Has the recent measles outbreak in the United States swayed your opinion? What concerns do you have about immunizations? What concerns do you have about the diseases vaccines are designed to prevent?”
In response to the Jenny McCarthy style journalism I found, I chose to write this note directly to the reporter. Here it is. I hope she can make amends later for her journalistic transgressions and learn a little bit more the history of communicable diseases in the Oregon, where diseases like smallpox literally helped to wipe out many Native American communities before most white settlers arrived.
Letter Sent Feb. 4, 2015, by email:
Ms. Gabrielson: What exactly were you and your editors possibly thinking framing the public heath issue of a scientifically proven health intervention (MMR vaccination) that is used globally to save lives by giving precedence to perpetrators of junk science whose ideas have now been thoroughly disproven by peer-reviewed, country-wide, and massive population-based studies showing absolutely no proven link to autism and the MMR vaccine?
Do you even understand what a population-based study is? Do you understand statistical significance or P-values? Do you understand the perpetrator of this bogus original article has been thoroughly debunked? Do you even know the history of this state where infectious diseases literally wiped out entire Native American villages on a scale that makes Ebola look like a mild chest cold?
If I were to start claiming, say that European Jewry was responsible for causing World War I and helped to defeat Germany, would you print an article with a headline talking about, tell us your thoughts on the debate about Jews’ role causing WWI. Would you open up your comment blog to Nazis and skinheads who will speak with utter sincerity using widely disproven racial eugenics theory that have the exact same scientific validity as those perpetrated by former Playmate Jenny McCarthy?
Wow.
Maybe you should learn about what happened to Native Americans in Oregon barely 160 years ago, due to smallpox and malaria. Maybe that might inspire you and your paper to use your brains. Promoting profits for junk reporting at the expense of public health is rather disgraceful if you ask me.
Few books stay with me for long. I read them and give them away. One has stayed on my bookshelf, now for 26 years. That book is Dr. Stephen Bezruchka’s The Pocket Doctor. First published in 1982 by the Mountaineers, this pocket-size reference, now being published at a bit more than 100 pages, is exactly what its title implies. It is a guide to help a traveler cope with illnesses many people in the developing world face daily. You can buy it online from many vendors, like Powell’s Books.
Cover of the second edition, 1988 version of Dr. Stephen Bezruchka’s The Pocket Doctor (personal copy).
I credit this book for saving my bacon and mental health on several best-forgotten nights. It helped me cope with medical problems that are normal for hundreds of millions of residents globally, and for me something I did not experience back in the comfort of the United States. But I am not the only writer and traveler who praises Bezruchka and his book.
Why many trust Bezruchka’s work
Bezruchka is a Canadian-born former emergency-room doctor trained at some of the nation’s best universities (Standford, Harvard, Johns Hopkins). He has both an MD and MPH. He has worked with medical specialists in the developing world, notably Nepal for 10 years. He also has written a great guide called Trekking in Nepal, which I used back in 1989. Today he is a lecturer on global health at the University of Washington School of Public Health (UW SPH) and a nationally recognized advocate for health care reform to improve public health outcomes and to eliminate health and income inequality.
I have taken this book with me now to three continents: Asia, Africa, and South America. I just cannot say goodbye to it, even when my developing-nation jaunts seem fewer and fewer.
The advice it provides has helped me to self-diagnose all manners of common gastrointestinal disturbances, such as food poisoning (nasty and scary in a crappy place), dysentery, and common diarrhea. I also used it to help me obtain the necessary medicine for what I still believe was malaria, which I had in Kigali, Rwanda in 1997.
With this book in my hand, I felt I could handle the predicaments that afflict visitors from developed countries to less-developed areas. In my 1988 published version, 13 pages are devoted to common drugs and medicines that address typical maladies, such as the antibiotic ciprofloxacin, to tackle infections, with information laid out in a table on a drug’s use, likely place of need (city, remote, “third world”), form, and dosage.
Basic health care advice can be fun with good writing
Bezruchka’s writing is straightforward and direct. In his chapter on drugs, he begins his recommendation with a simple message: “Remember that drugs, though valuable, are not a cure all.” He provides advice on assembling a medical kit, working with doctors at home and abroad, and dealing with major sources of health problems—namely, food and water.
Bezruchka also highlights a major global health issue that is more severe than microbial agents, trauma from vehicle accidents. “Trauma, especially that caused by motor vehicle accidents results in the majority of disability acquired in developed countries,” writes Bezruchka. “This is even more true in third world countries. Trauma causes more disabilities to travelers in foreign countries than all the exotic diseases put together.” That observation remains true to this day, as shown in global health data.
Faculty photo of Dr. Stephen Bezruchka, courtesy of the University of Washingston School of Public Health web site.
But there is much more. Rabies? Check. Animal attacks? Covered. Ticks and leeches, fever, rashes? All addressed. The two-page section, in my old and battered version, on dealing with stress in less-developed nations is a classic summary of what many first-world travellers experience.
“If the culture shock of a third-world setting with its attendant poverty and hopelessness have you in despair, take steps to improve your psyche,” writes Bezruchka. “Seek out help, another traveler, or a religious organization or individuals.”
Bezruchka even has sections on death and how to cope with returning from travels with an illness. I definitely experienced lingering issues when I came back and took this advice to heart.
Meeting Bezruchka later in life
When I first met Bezruchka in person during my studies at the UW SPH, I mentioned how much I enjoyed his book and used it frequently in Nepal. I even mentioned how enterprising Nepalis had published black-market copies of his book they were peddling on the streets in Kathmandu. As I recall, he considered that a compliment to the value of his work.
Sometimes small and perfectly executed creations are ones that have the most impact. In Bezruchka’s case, there is far too much to choose from to say what is best—from published papers to advocacy to mentorship of future health leaders. I will submit this still fine tome as work that stands the test of time and proves that small is often better.
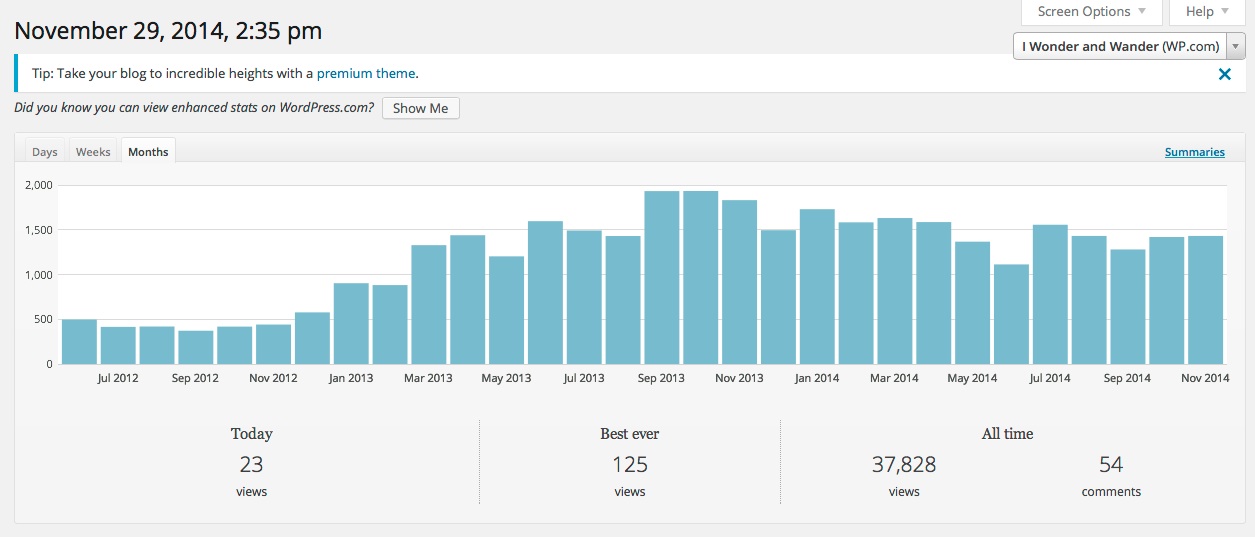
I began this blog in March 2012 to share my perspectives on public health issues and to integrate multiple disciplines and perspectives that the traditional public health field either is not doing or does not want to do–such as speaking with moral clarity on the public health threat posed by firearms in the United States.
I took this screen snapshot of my dashboard on Nov. 29, 2014.
My blog has had nearly 38,000 page views as of late November 2014. This means this web site is getting more visibility and traffic than many published papers by academic researchers. Many of their peer-reviewed articles will never be seen because they are behind a firewall run by for-profit companies that prevents publicly-financed research from reaching policy-makers, the popular media, and the public who pays for the research.
To celebrate the eventual “fall of the wall,” meaning the for-profit firewall that is stifling innovation and blocking research from having greater value to the public, I am going to highlight a few of my more popular public-health articles based on visitors and page views.
I think it is time to start dismantling the firewall and to start telling public health’s story with more traditional storytelling techniques, with more creativity that bridges disciplines, and with an eye on upstream advocacy.
The articles I shared above do not follow the traditional model of public health writing or practice, and some challenge the current U.S. models as broken and even morally bankrupt, particularly regarding the historic deathly silence by public health leaders at the local and national level and at universities in the face of firearms-related violence in the United States.
So if you landed on this page and find yourself within the claustrophobic walls of academia as a student, grad student, or faculty member, and you have not been exposed by your peers or the faculty to the value of blogging, here 38 reasons why you need to get off your freaking butt right now and get to work. If you work in a public health office and your office is not actively using social media because of out touch managers and your office is not advocating with lawmakers, you need to show leadership and become the change you want to see and not wait for others to do it for you.
Yes, it is time to think creatively and innovate and challenge the old guard whose ways are failing to make a greater impact.
My list of blogs/articles may be updated as I continue to publish more of them. I am now using this blog to discuss organizational behavior, multi-disciplinary research, and stories based on personal and professional experiences as the starting point for discussing larger issues. I hope you come back from time to time to check out my articles. Thanks.
(Note, I am publishing this blog post as both a page and post on my blog.)
“But despite what you may think, good luck is more dangerous than bad luck. Bad luck teaches valuable lessons in patience, timing, and the need to be prepared for the worst; good luck deludes you into the opposite lesson, making you think your brilliance will carry you through. Your fortune will inevitably turn, and when it does you will be completely unprepared.” … Robert Greene, The 48 Laws of Power
During a recent outing to one of Seattle’s many brewpubs, I swapped stories with my good friend about hospital visits. Most people I know have had them, and a rarefied few have not. In my case, I have been hospitalized at least a half-dozen times, mostly for stitches, but also worse.
I told my friend some of my greatest learning moments came with contemplation lying in a hospital bed. There is nothing like pain one feels in the ugliness of a hospital room to focus the mind and to allow one to make sense of all the things that preceded the unforgettable trigger moments.
South African born psychiatrist and author Norman E. Rosenthal
South African born psychiatrist Norman E. Rosenthal has written a book on this theme called the Gift of Adversity. Thinking back on his own Apartheid-era life, surviving a near fatal stabbing, and his professional experiences, Rosenthal argues that innovation, resilience, and understanding emerge from our own adverse experiences and by gaining wisdom from those hard times. Writ large, economists will even refer to collective behaviors among entire generations, such as young people who came into adulthood in the Depression era, and whose lifelong buying patterns and decisions to live more austerely can be quantitatively measured.
Using examples of individuals who endured suffering yet who came out stronger, Rosenthal sees opportunity in these struggles for all of us. “Well, when adversity comes, the last word that comes to mind is gift, because it just looks like an unmitigated disaster. But, how many times have you heard a friend or somebody say, ‘You know, at the time, it seemed terrible, but in retrospect, it was for the best.’ … The first step is really to accept that the adversity has happened. … We have to somehow come to terms that it really has happened. Then, we have to analyze the situation, every adversity is different, and respond accordingly.”
My own experiences mirrored these points, almost too perfectly. Both involved small misfortunes with lifelong rewards.
Lesson No. 1: When I was 14 and not fully mature, I did something that was likely one of the dumbest acts of my life. I will not say exactly what it was, but it substantially disrupted life at my often-violent and chaotic junior high school, in University City, Mo. I was soon on my way for an expulsion as the second-to-last-day of classes was ending in June 1979.
Coming back to campus I encountered four guys who I did not know. At least three were students. The other may have been a high school student. He was older, a guy with a cast. They were tough. I was not. They were experienced in the art of violence. I had few such fighting skills. They were skillful manipulators, and I fell for small talk that drew me close. It turns out one of them had been blamed for the incident. That is the story I heard second-hand, and the group was bent on physical vengeance.
I do not remember everything that happened, but I do remember feeling a floating feeling. I was cold-cocked in the face by one of the four wearing a cast. I was bleeding profusely from a cut on my eyelid and could not see out of my left eye. I was lying on the ground not sure what had happened. I felt warm blood on my hand.
I remember the four of them mocking me and telling me if I was happy now about having the heat fall on them. It was a perfect example of the violence I had witnessed many times before at this school, often with the tense black-white racial undertones, and I am sure that tension influenced this assault too. They walked away, never having been arrested, never having been questioned by anyone, ever.
Insult piled upon injury. I had to go back to school, get kicked out by a furious principal who did not express any concern about me having just been assaulted on school grounds, and then have teachers sign my expulsion papers. One thug laughed at me in the hall and yelled, “What happened to you.” I shot back, in my un-masculine voice, “What do you think happened.” He turned cold, came close, and threatened, “Yo, want another one, mother fucker.” Luckily I walked away from that one.
I stayed at this hospital for nearly a week after I was assaulted and nearly blinded in my left eye, which proved to be a great learning moment.
My mom, a new teacher that year in the same district, took me to the emergency room in Barnes Hospital in St. Louis, where I was put into a shared room and monitored. My eye pressure was dangerously high because vessels were ruptured from blunt trauma, and I was at high risk of blindness in my left eye. The doctors prescribed having both eyes covered for more than a week to keep them from moving, lying in a bed, and having no physical activity.
I remember the slow passage of time and mostly the sounds of the ward, the voice of my few visitors, and the stories of a young man next to me going into eye surgery, not sure what would happen.
The school principal came once, talked briefly, and somehow waived my punishment as a result of being a violent crime victim. He never told me or my mom what the school or school district had done to investigate the assault. My mom told me years later she was too afraid as a new teacher to make waves with her new employer. No police officer ever took my story. The whole thing was wiped under the rug.
Lying there, in a flimsy hospital gown, feeling like needles were piercing my eyeball, I came to the realization of how precious my sight really was, and how close I had flirted with genuine disaster.
Lesson Learned: This was the clearest teaching moment ever in my life. Never, ever, do stupid things. Such acts have unforeseen consequences, particularly things that put you in a weak position with uncaring bureaucracies and with men who use violence to settle a score. If you act badly and unwisely without thinking, the sword of blunt justice will be swift, and it will be lasting. Also, without any allies or friends, one can be quickly abandoned by any organization if you are perceived as lacking advocacy skills and are vulnerable. So, do not present yourself as weak or easily exploited. Finally, and most importantly, always know exactly who you are dealing with when you confront strangers in strange circumstances. Trust your instincts, and keep your wits about you, always. Your instincts will always know who is a friend and who is a foe. Worry about bruised feelings later, from a safe distance.
It took me a whole summer to recover, and I could not engage in full physical activities for three months. I wore an eye patch half the summer. Decades later, I still have damage to the back of my eye that my most recent visit to an optometrist confirmed. He could see the damaged areas after my pupil was dilated.
Lesson No. 2: In my last month of my journalism master’s program at the University of North Carolina at Chapel Hill in July 1993, I was playing pickup soccer at the UNC-CH campus. It was supposed to be friendly, but of course men are fiercely competitive. A guy who I was marking intentionally head-butted me with the back of his head into my face. He broke my nose instantly, and it began to bleed profusely. I walked myself to the UNC-CH hospital, as it was close by.
This is how I looked shortly after my nose was broken and then reset in July 1993.
I waited about three hours for a resident to attend to my situation. The plastic-surgeon-to-be had been up about 28 hours and was in a terrible mood. After shooting cocaine painkillers into my nasal cavity area, he stuck a metal rod up my nose and proceeded to move things back into place. I recall screaming like a wild animal so loudly that it clearly disrupted patients in the entire wing. The exhausted and overworked resident was furious with my uncooperativeness, as he called it. He stuck the rod back in and went back to work.
A nurse came in and saw the procedure. She simply held my hand. I stopped crying. I instantly calmed down. My level of pain subsided dramatically. The compassionate act of human touch proved more powerful than any medicine. After the resident stuffed both of my nasal passages with some sort of medical gauze, I thanked the nurse. She gave me a caring look that said, everything’s going to be OK.
That night I wrote a poem about the war in Bosnia, then raging at the time, and I put my small problem into a larger perspective of suffering felt more severely by others around the world.
Lesson Learned: Human compassion and human touch are among the most powerful healing agents in the world, often more powerful than medicine and actions of medical specialists. The mind, when it needs to, can calm down and can process a stressful situation. Set the calming effect in motion, and show mindfulness of yourself and others who may be less fortunate.
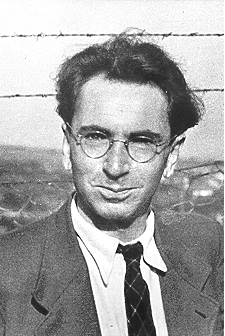
Comment: Author Rosenthal, who sees the importance of adversity, profiles the late Austrian neurologist and psychiatrist as well as a Holocaust survivor Viktor Frankl. He was the only member of his family to survive the genocide, staying in four different camps, and went on to receive acclaim for his widely read treatise called Man’s Search for Meaning, original published in German in 1946 Trotzdem Ja Zum Leben Sagen: Ein Psychologe erlebt das Konzentrationslager.
Holocaust survivor, psychiatrist, and author Viktor Frankl
Frankl’s own horrific experience taught fellow psychiatrist Rosenthal critical lessons also, that one can find meaning even in the midst of terrible adversity and that no single group of people is pure good or evil. Both types of people can be found in all groups, everywhere.
“It did not really matter what we expected from life, but rather what life expected from us,” wrote Frankl. “Our answer must consist, not in talk and meditation, but in right action and in right conduct. Life ultimately means taking the responsibility to find the right answer to its problems and to fulfill the tasks which it constantly sets for each individual.”
In no way did anything I experience come close to the challenges Frankl and other tough and lucky individuals have endured from such crimes.
I do know that in my case, my invaluable teachers came disguised as sterile wards and rooms of hospitals, giving me opportunities to contemplate larger truths. In one case, I created my own folly but could use my intellect to evaluate my mistakes. I also benefitted from being in hospitals, where I seldom felt kindness and felt great stress and also fear. This was clearly a place to avoid at all costs. I was doubly motivated to stay healthy—mind, body, and soul.
The wisdom I gained at those small junctures far exceeded anything I received in any university setting. As Robert Greene’s opening quote aptly notes, our bad luck prepares us for misfortune and gives us the strategies to overcome the roadblocks we build for ourselves or encounter from others. Those who are blessed mostly by good luck will eventually see their luck change, and when they do, they will be overtaken by those who have adapted and learned already.
So be thankful for those learning moments. They are your teachers, and you profit immensely by employing that knowledge wisely in the future.
Even four days after the best World Cup final I have ever seen, I am still brimming with the euphoria that only seems to accompany el jogo bonito (the beautiful game) in its finest form. What a spectacle it is. Teams from 32 nations around the planet vie for supremacy of being called the world’s best team. Remember that word, T-E-A-M.
Germany’s relatively small-sized but experienced captain, Philipp Lahm, captured it best after the final game against Argentina. “It’s unbelievable what we have achieved,” said the Bayern Munich defender. “Whether we have the best individual player doesn’t matter at all, you just need to have the best team.”
This Tweet was widely re-Tweeted after Germany crushed Brazil 7-1.A great shot published on game day of the victors celebrating their win in the biggest sporting event in the world.
I watched more matches than I planned to, and found myself swept away, as always, in the massive melodrama that captures the world’s attention every four years. This year was no exception.
Uruguayan Luis Suarez bit an Italian opponent like a zombie.
The host team lost in the biggest knockout-round blowout ever in the Cup, 7-1, to winners Germany after its star player, Neymar, had his back broken.
One nation, Cameroon, was alleged to have thrown a game. And of course there were countless displays of sheer athletic brilliance like goals scored by Colombia’s James Rodriguez and would-be goals blocked by U.S. keeper Tim Howard.
More than a game … a social media spectacle of historic proportions
An Internet meme beautifully shows how U.S. keeper Tim Howard blocked the goals against Belgium.
It is estimated the final match that saw Germany top Argentina in a 1-0 nail-biter decided in the 113th minute drew about 26 million viewers in the United States. In Germany, about 35 million fans watched the game on TV, not to mention public viewing areas. Globally, around the world about 1 billion may have watched, but I suspect the number was higher. I doubt they count small bars in rural China and Africa and other remote spots.
Mario Gotze scores the winning goal against Argentina, as shown in possibly the penultimate game photo of the tournament.
And what a great final game it was, with a brilliant end. Germany’s André Schürrle darted down the sideline and sent a perfect cross to teammate and fellow late-game sub Mario Götze. Super Mario trapped the volley with his chest and blasted the ball to the side of the net. GOOAAAAALLLLLLL!!!!!!!!!
Where I was watching the game in Seattle at a neighborhood center, half the room went nuts, with orgiastic screaming. Half the room cheering for a great Argentina side fell stunned silent. That is pure World Cup emotion, and there is absolutely nothing else like it in the world. Period.
Some researchers have said events like soccer have a hormonal factor in a brain peptide, oxytocin, that research shows promotes positive intersocial relations. It is called the “love hormone” because it makes people like one another, especially in intimate relationships like mother and child. Research shows that players’ exhibitions of emotions like happiness and confidence, as in after a great play or goal, can be contagious, when a person’s excitement triggers biochemical reactions in onlookers’ brains.
That is precisely what happened at the same moment around the globe when everyone watching the game on TV and giant screens saw the emotions on the German team members’ faces after the goal.
Bam, oxytocin discharge, followed by social media frenzy.
Social media globally turned into a raging wildfire. Twitter sent more than 600,000 Tweets a minute after the match on July 13 and more than 670 million Tweets by the next day, more than ever before in its short history. On Facebook, there were 280 million interactions such as posts, likes, and comments—the most for a sports event.
It was a sports event and a social media happening of historic proportions at the same time. Small wonder German Chancellor Angela Merkel was at the stadium hugging the sweating German team one by one, and even posed for a selfie with starter Lukas Podolski, and soon that Tweet blasted around the world.
Lukas Podolski tweeted this selfie of him and the German leader right after the game, in a Tweet seen ’round the world.
So it is no boast the singularly most important global event of the past month was the Cup, despite all of the raging conflicts that continued during its course. People the world over adore it, and go crazy over it, and weep and moan over like, like the entire 200-million-person host nation of Brazil did after the German team brutalized the host team 7-1 in the semi-final blowout that was a record-breaker of historic proportions.
Why the game is great, and the Cup is greater
Professionally, the game is easy to grasp. It has simple rules, a 100 meter pitch, three referees, and 22 men making up two teams who are fiercely competing for the title of best national team on the planet during Cup time. I love the Cup because it, more than anything else, is a common denominator that I have with someone in remote Greenland; and Munich, Germany; and Kampala, Uganda; and Rio de Janeiro, Brazil. No matter where I go, I can always talk about the Cup, and I will have a well of good feelings and excitement to draw upon.
This is one of the best shots after the game: Lionel Messi of Argentina is consoled by Germany’s Bastian Schweinsteiger.
What I most liked about this year’s final game was the near-perfect match of two really outstanding teams.
On one side, you had the world’s greatest player, forward Lionel Messi of the elite club Barcelona, who was surrounded by a team that got stronger and more cohesive as the tournament progressed. They were matched by Germany, which lacked the flash and brilliance of Messi, but who had perfected what football commentators called a system of teamwork and cohesion. (Granted this system is strongly supported by the nation’s football federation.)
In fact, the two best teams showed up in the Maracana stadium, and both played great team soccer.
Passing was strong, there were not many dirty tackles, and both sides had great scoring chances, only to see them squandered. Argentina actually blew three golden opportunities, including one by Messi inside the box, with no one close enough to shut him down. With the exception of two horrible concussions during the game, one to each side that later forced commentators to blast FIFA’s system and led to many calling the contest the “Concussion Cup,” the game was without flops or debilitating injuries.
Despite the excesses and corruption of the world football governing body known as FIFA, for me, Brazil’s 2014 Cup was a great reinforcing example of the power of teamwork.
Organizational behavior theorists have long championed Naval researcher Bruce Tuckman’s famous four stages of group performance from his seminal 1965 article (Development Sequence in Small Groups): forming, storming, norming, and performing. When groups are clicking as a unit, they can achieve well above their own individual abilities and, if really good, as in high-stakes activity like conflict and sport, achieve greatness and victory.
As someone who played soccer most of my life from youth to middle-age, I can attest to the power of teamwork and how effectively groups with lesser abilities can overcome better opponents who do not have that cohesion.
The ultimate team player, Miroslav Klose of Germany
Germany had the team magic. It was obvious the whole tournament. There were great plays by the German team stars like Thomas Müller, even very great plays like Götze’s winning blast, but all of the German team members contributed to their success. The perfect example was forward Miroslav Klose, 36, and veteran of four World Cups and likely the most underrated player in the world. He scored two in the Cup, both lovely.
In the victory over Brazil, the “poacher” scored his 16th Cup goal (see all here), more than any other player in the history of the Cup. He did it as he always did, getting great service from his teammate, and always following up when his first shot was blocked.
This photo captures a perfect moment: forward Miroslav Klose scores his 16th World Cup goal against Brazil, a record and a lasting tribute to a great team player.
Klose is not pretty. He is not charismatic. He does not smile often, and he is a quiet family guy. In fact, his lack of flash allows defenders not to respect his killer instinct as a finisher. Most of all he has succeeded in making history by being part of a great team that worked relentlessly at being the best at what it did, and then did it in the highest possible stakes game there is in the world.
My hat is off to the German, and Argentinean, teams. Thanks for making this Cup memorable and for showing how two great teams play the best game in the world.
I recently saw the Brad Pitt zombie action vehicle, World War Z.
Brad Pitt goes toe-to-toe with the zombies and saves humanity in his public health swashbuckler, World War Z. Way to go, Brad!
It is actually not a bad zombie apocalypse movie, as zombie apocalypse movies go. Brad saves earth, and a lot chattering, undead humans get shot and blown up. It also is a fairly straightforward public health film, which foretells horrific calamity to humans because of some possible viral outbreak that could kill much of humanity. (If you are not worried about this, then perhaps read up on the recent Ebola virus outbreak that is causing legitimate fear and even panic in West Africa.)
Though I have no data to back up this claim, I am guessing more people around the world have learned about viruses and the threats they can pose to population and human health from such films than anything ever produced by a national or government health agency.
I also believe that public health advocates need to fully embrace the “Brad Pitt saves the world from zombies” approach and copy it, and also use such storytelling techniques to mobilize public understanding of public health issues, from the importance of vaccinations to the woeful underfunding of public health in the United States.
Can the 10th man save public health and humanity?
What I most liked about WWZ was its exploration of the concept of the 10th man, which is used by Israel’s security apparatus.
In the film, Israel had prepared for a zombie apocalypse because it had institutionalized a non-consensus decision-making safeguard. A Mossad security official character, Jurgen Warmbrunn, explains to Pitt’s hero that because of Israel’s pre-nationhood and post-nationhood catastrophes, including the Holocaust and the Yom Kippur War, one person in a decision-making group has to take the contrarian view if all nine of the others reach consensus. In Israel’s experience, failure to do so could lead to extinction. Then that person, the 10th man, must put the alternative view forward, with the larger goal of promoting the interests of the organization, country, or collective. That is why Israel in the film was ready for the zombie horde. (Click on the video snapshot below to see the clip on YouTube.)
In science, this happens all the time. Scientists and statisticians do this by attacking the null hypothesis that seeks to disprove their theory they believe to be true.
But I am more interested these days in how this may work in organizations outside of intelligence circles and defense, where mistakes can cost many lives and national security, and how organizations can incorporate 10th man decision-making. Can the contrarian view be protected and even respected in organizations that do not allow for rigorous debate about choices that have implications for the public’s well-being?
Kill the messenger and avoid demonstrating leadership?
We know the popular legend of the archetypal messenger who loses his head when he brings bad news to the king. I was a newspaper reporter, and I have lived this in a mild way, having been threatened with a lawsuit by a corrupt community leader and vilified by autocratic public officials who wanted to have their malfeasance remain hidden. A new movie called Kill the Messenger, focusing on drug running by the Nicaraguan Contras during the Reagan presidency, explores this issue in-depth.
Italian physicist and mathematician Galileo was deemed a heretic and tried for his promotion of the Copnernican or heliocentric view that the earth orbits the sun and that the earth is not the center of the universe.
In fact, the phrase “kill the messenger” is known and understood globally, and for good reason. Many people know that organizations and human nature prevent good people from offering alternative views that challenge authority and orthodoxy. Some like Galileo, who offered a view the earth was not the center of the universe, turned human understanding of man and God on its head, and he was ex-communicated and not forgiven for more than four centuries by the Catholic Church.
So how can organizations, like public agencies such as health departments, create safe environments to allow for alternative views to flourish, for the purpose of improving decision-making internally. This is no easy fit, as these are hierarchical by design, and I have yet to hear how alternative decision-making works in them in a real-word basis.
In organizational theory, Peter Senge’s so-called “learning organizations” may be a model, but that is not really the built-in acceptance of a 10th man contrarian. Of course CEOs, companies, and consultants aplenty try to allow contrarian views because the endgame for them is profit maximization and success of the firm. In the world of intelligence gathering and organizational behavior. failure has been dubbed “group think.”
Getting back to our popular public health film trope, the zombies
Personally, I would love to see public health agencies, top to bottom, hire and fund the bright and brilliant artists who are creating manga comics and who are making manga comic-styled videos. And it is no surprise some manga comic artists have been hired and there are positive results. I have seen one video already, produced by the outfit called the Global Health Media Project. The group published a gritty portrayal of how lethal cholera can be, as a means to promote global education against its spread. You can watch the video below by clicking on the image.
What would a campaign that promoted immunizations and targeted the promoters of anti-vaccination deniers look like if it were entrusted to artists who can tell riveting stories linked to movies, like the three clips below that accompany Will Smith’s I Am Legend zombie apocalypse thriller?
Check them out and see what you think–click on each screen snapshot to see clips on YouTube. Would there need to be a 10th man pitching these ideas inside the proverbial boardroom saying this would be a better investment of prevention dollars than methods that may have yielded no measurable results, ever?
One thing I have never shaken since my days as a rookie reporter is my penchant for calling out the obvious. This is one of the sacred duties of the press: to speak truth to power. This also means calling a spade a spade, and bullshit for what it is, and what it smells like.
Anyone who has ever worked in the business of reporting news and telling facts knows this is one of the press’s sacred trusts—and myths—and the clearer we are in doing that, the better our society is from having that unbiased information.
I captured these various images on Google when I typed in a few keywords, and clearly this concept has a lot of widespread acceptance by people who know a cow patty when they smell one.
Today, I stumbled on Marcy Wheeler’s blog, the Empty Wheel, which tackles many hot-button policy issues. Last year she blogged about climate change in a piece called “The Cost of Bullshit: Climate Change, National Security, and Inaction.” She pointed out that the cost for maintaining the status quo was too high, even when major government agencies from the Department of Defense and the Department of State concluded that the issue was a critical concern to U.S. national interests. Yet, no actions were being taken by the government, and all of the reports on the emerging crisis were “mere bullshit—more wasted government employees’ time and taxpayer money.”
Sure easy for a blogger not on the payroll to diss hard-working public workers and policy-makers, right? Or, is Ms. Wheeler simply calling out the obvious, like reporters have always done, or thought they were doing.
Will a public health fad meaningfully address the main killers of Americans?
The cost of bullshit has been on my mind late, particularly regarding public health jargon that inflates busy-looking arm-waving, but does not change reality.
For me, one of the most frustrating aspects of working in the public health is the field’s faddish way it labels its collective actions to address chronic disease issues, such as obesity, using fancy sounding concepts like “policy, systems, and environmental change.” Mon dieu, what big words, what big ideas.
This is an expression coming from the top, from the venerable U.S. Centers and Disease Control (CDC), to explain national efforts to tackle the monster that is chronic disease—the leading causes of death in our ever-fattening and ever growing income-unequal country.
These diseases kill seven in 10 Americans, and of the CDC’s meager budget of under $7 billion for our national public health effort is a mere drop in the bucket compared to other priorities of the $1.2 trillion national budget that is so-called “non-discretionary spending.”
The Congressional Budget Office released this infographic on government spending and revenues for 2013. Go here for original: http://www.cbo.gov/publication/45278.
The CDC still estimates 18% of U.S. GDP spending is on healthcare, and a third of it at the place where the most outrageously overpriced and at the same time least effective primary care interventions can take place—hospitals.
So what do public health officials do, when faced with a handful of breadcrumbs thrown to them from Congress? They invent concepts that make it appear that public health is doing something, when there is little or no clear evidence population benefits are accruing based on investments at this level in the large ocean. Yes, I am talking about the catchy and jargon-laden ideas like “policy, systems, and environmental change.”
This is a hodge-podge of activities that encompass everything from starting farmers markets to promoting smoke-free buildings. Here are a couple of definitions I randomly found from some online sources:
State of Mississippi: “Our environment and the policies and systems in it shape the pattern of our everyday lives and have a profound influence on our health. The design and walkability of communities, the availability of low-cost fruits and vegetables, and the smoking policies in our workplaces have a direct impact on our physical activity, diet and health.”
State of Maryland: “Policy, systems, and environmental change (PSE change) refers to public health interventions that modify environments to provide healthy options and make healthy choices easy for everyone.”
Fairfax County Virginia: “Policy, systems and environmental change is a way of modifying the environment to make healthy choices practical and available to all community members. By changing laws and shaping physical landscapes, a big impact can be made with little time and resources. By changing policies, systems and/or environments, communities can help tackle health issues like obesity, diabetes, cancer and other chronic diseases.”
Budgets for this kind of intervention exist in most public health jurisdictions, and public health leaders are doing to the talk, because they have so few funds to do the walk. But public health experts end up playing in a small sandbox when these investments are measured against other spending, and then we spend a lot of time trying to convince ourselves through published papers, webinars, conferences, and the like that this is working. The illusion is powerful, like the illusory power of the Iron Throne in the Game of Thrones, except the shadow from a fad still does not make meaningful change when the numbers are crunched and the costs are calculated regarding chronic disease.
From the Game of Thrones, a lecture on power and illusion, for Westeros and beyond.
Public health departments who get funding through competitive grants from the CDC spearhead these efforts and then spend extensive amounts of time documenting their work trying to prove the bread crumbs made a difference to the overall health crisis facing Americans.
About $200 million was doled out from 2011 and 2012 through an effort called Communities Putting Prevention to Work (the amount initially announced in 2010 was about $380 million). In one case, Public Health-Seattle & King County published findings that show its CPPW-grant-funded efforts in schools cut youth obesity in specific schools by 17 points. Great job, except the funding was not permanent and it was not renewed when the grant ran out. The program is now in the past tense.
In 2014, public health professionals learned another funding source, the Community Transformation Grants, which also promote the policy, systems, and environmental work, is being cut too. Some can argue the money is being allocated to other programs that tackle chronic disease, focusing on heart disease and diabetes.
More musical chairs without really changing the big picture again?
I do not mean to belittle the work of public health people doing this work. They are my colleagues. I respect them. And the work being done, like promoting activities to reduce tobacco use and get more people eating healthy food, should be continued.
But as a field, I am convinced this type of work is self-delusional because it hides the nasty realities of how much larger issues shape the public’s health, such as how transportation budgets are allocated, how cheap petro-based energy is spurring obesity in measurable ways, how legislation is crafted by special interests at the state and federal level, and how the principle of health care is considered a privilege not a right in the United States. (In Denmark, by contrast, the public funds about 85% of all health care through taxes, and the system is rooted in both law and a social contract that is premised on system where all citizens are provided free and equal access to quality health care.)
Emilia Clark, mother of dragons in the smash HBO TV series Game of Thrones, is a good visual metaphor of what public health is not in the bruising world of budget appropriations at the state and federal levels of government.
The nasty realities we do not want to think about, using a contemporary TV metaphor, would be what happens when the violent kings of Westeros cut deals and cut heads, to maintain order in that mythical, lovable place with White Walkers, a giant ice wall, and fire-breathing critters. Mother of Dragons, public health is not, that is for sure!
I imagine a new fad will emerge in public health in the next three years, like it does in management. We might change the concept, but we likely may even have a smaller piece of the government pies.
No, public health jurisdictions cannot stop working until we see changes on these fronts. But the more we in public health delude ourselves that we are making a difference with scraps from the table, the more easily we are duped into accepting that the larger model is as it should be, and how it shall always be.
We will continue kvetching about farmers markets and soda machines, but not moving in a rigorous way upstream, where budget deals are made with transportation dollars, for starters. And I think we have to start being honest with ourselves about what we are accomplishing in the sandbox and whether this is the best use of our meager and diminishing resources.