I began this blog in March 2012 to share my perspectives on public health issues and to integrate multiple disciplines and perspectives that the traditional public health field either is not doing or does not want to do–such as speaking with moral clarity on the public health threat posed by firearms in the United States.
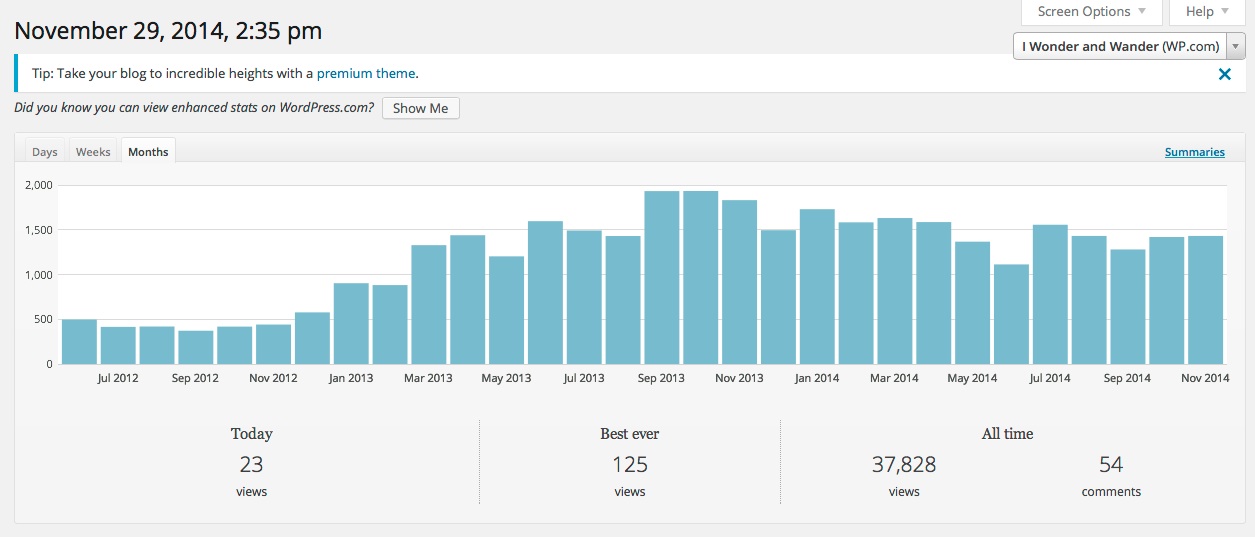
I took this screen snapshot of my dashboard on Nov. 29, 2014.
My blog has had nearly 38,000 page views as of late November 2014. This means this web site is getting more visibility and traffic than many published papers by academic researchers. Many of their peer-reviewed articles will never be seen because they are behind a firewall run by for-profit companies that prevents publicly-financed research from reaching policy-makers, the popular media, and the public who pays for the research.
To celebrate the eventual “fall of the wall,” meaning the for-profit firewall that is stifling innovation and blocking research from having greater value to the public, I am going to highlight a few of my more popular public-health articles based on visitors and page views.
I think it is time to start dismantling the firewall and to start telling public health’s story with more traditional storytelling techniques, with more creativity that bridges disciplines, and with an eye on upstream advocacy.
The articles I shared above do not follow the traditional model of public health writing or practice, and some challenge the current U.S. models as broken and even morally bankrupt, particularly regarding the historic deathly silence by public health leaders at the local and national level and at universities in the face of firearms-related violence in the United States.
So if you landed on this page and find yourself within the claustrophobic walls of academia as a student, grad student, or faculty member, and you have not been exposed by your peers or the faculty to the value of blogging, here 38 reasons why you need to get off your freaking butt right now and get to work. If you work in a public health office and your office is not actively using social media because of out touch managers and your office is not advocating with lawmakers, you need to show leadership and become the change you want to see and not wait for others to do it for you.
Yes, it is time to think creatively and innovate and challenge the old guard whose ways are failing to make a greater impact.
My list of blogs/articles may be updated as I continue to publish more of them. I am now using this blog to discuss organizational behavior, multi-disciplinary research, and stories based on personal and professional experiences as the starting point for discussing larger issues. I hope you come back from time to time to check out my articles. Thanks.
(Note, I am publishing this blog post as both a page and post on my blog.)
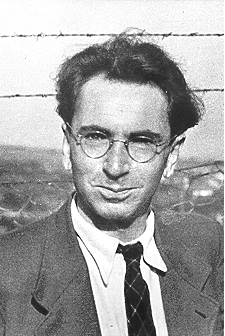
This photo of Viktor Frankl was taken shortly after his liberation from the Nazis in 1945.
Renowned psychiatrist, philosopher, and writer Viktor Frankl stands as a giant among 20th century thinkers. The Austrian-born Frankl (b. 1905, d. 1997) was a psychiatrist whose life was transformed by his experiences as a Jewish prisoner who survived the Holocaust and internment at the Auschwitz death camp and three other German concentration camps.
With the exception of a sister, all of his immediate and extended family and his beloved wife were murdered by the Nazis. From the aftermath of this horrific experience, he embarked on a life’s work that provided deceptively simple but remarkably clear ideas that literally provide a framework on how all people can live meaningful lives.
Frankl survived his brutal internment, which should have killed him, by seeing a purpose in his ugly reality and by taking control of his responses to that experience with positive actions and a mental attitude that ensured his survival and also his outlook on life and his fellow man and woman. His simple ideas offer no shortcuts, and they uncomfortably place each person in control of how they choose to respond to life’s challenges, even ones as unforgiving as genocide and mass murder.
Frankl proposes all of us are motivated to seek a higher purpose, even when our circumstances are as cruel as a death camp surrounded by barbed wire and vicious men armed with machine guns. Frankl writes: “Man’s search for meaning is the primary motivation in his life not a ‘secondary rationalization’ of instinctual drives. This meaning is unique and specific in that it must and can be fulfilled by him alone… .” More than pleasure, more than material things, meaning motivates us all. It is our purpose for being.
Man’s Search for Meaning, a book that changed modern thinking
Viktor Frank’s seminal 1946 Holocaust memoir, Man’s Search for Meaning, has been translated into more than 20 languages, has sold more than 10 million copies, and is considered one of the most influential books among American book readers.
Frankl published those principles in his highly acclaimed and influential 1946 memoir, Man’s Search from Meaning, which today has been translated in more than 20 languages and has sold more than 10 million copies. It is considered among the most influential books in the United States, according to a Library of Congress survey.
He originally developed the framework for his sparse set of powerful ideas when he was practicing psychiatry in Vienna before the Nazi occupation and saw how he could help patients overcome their suffering by making them aware of their life’s calling. His treatise, stashed in his coat, was literally lost when he was imprisoned.
Later in his life, when he had achieved global recognition because of the widespread popularity of his bestseller, he was asked by a university student: “…so this is your meaning in life… to help others find meaning in theirs.” His reply was as clear and direct as the theory behind his therapy, “That was it, exactly. Those are the very words I had written.”
As one writer influenced by Frankl, Genrich Krasko, points out, Frankl’s ideas are more prescient today, given millions have no meaning in their lives, particularly in affluent societies: “Viktor Frankl did not consider himself a prophet. But how else but prophetic would one call Frankl’s greatest accomplishment: over 50 years ago he identified the societal sickness that already then was haunting the world, and now has become pandemic? This ‘sickness’ is the loss of meaning in people’s lives.”
Logotherapy, Frankl’s foundational theory
Frankl called his system logotherapy, derived from the Greek word “logos,” or “meaning.” It has been called existential analysis, which may over-simplify its scope. The philosophy and medical practice boils down to providing treatment through the search for meaning in one’s life. Its utterly basic but ultimately powerful foundational ideas are easily summarized:
Life has meaning in all circumstances, even terrible ones.
Our primary motivation in living is finding our meaning in life.
We find our meaning in what we do, what we experience, and in our actions we choose to take when faced with a situation of unchangeable suffering.
Frankl notes, “Most important is the third avenue to meaning in life: even the helpless victim of a hopeless situation facing a fate he cannot change, may rise above himself, may grow beyond himself, and by so doing change himself. He may turn a personal tragedy into triumph.” This latter point is particularly poignant, as it calls out the role that adversity can have in shaping us and our destinies and improving our character and our life’s narrative.
In short, no matter what circumstances we find ourselves, so long as we have a purpose, we can find fulfillment. What’s more, we are fulfilled by right action and by “doing,” not through short-term pleasure or narcissistic pursuits.
Frankl argues that meaning can be found in meaningful, loving relationships, in addition to finding it through purposeful work or deeds. In fact, it was the strong love of his first wife that kept him alive amid the unspeakable horrors of Auschwitz. He felt her presence in his heart and it literally let him live when others around him perished.
Frankl’s core ideas at odds with more ‘accepted’ health and mental health paradigms
Frankl’s ideas collide with behaviorist models, which show that conditioning will determine one’s responses—the proverbial Pavlovian dog or Skinnerian lab rat. By contrast, through his own experiences and those he observed treating depressed and suicidal patients before and after the war in Vienna, Frankl claims that “everything can be taken from a man but one thing: the last of the human freedoms—to choose one’s attitude in any given set of circumstances.”
When faced with a situation, we all chose. But our power is defined by our actions. “Between stimulus and response, there is a space,” he claims. “In that space is our power to choose our response. In our response lies our growth and our freedom.”
The concept of personal choice conflicts with extensive research that clearly documents how one’s environment, race, socioeconomic status, and more—the so-called social determinants of health (SDOHs)—shape one’s life more than one’s individualistic decisions.
A model explaining the social determinants of health.This photo of Viktor Frankl was taken two years after his liberation from the Nazis, when he returned to psychiatric practice to help people through his principles called logotherapy.
For two years, while earning my MPH at the University of Washington School of Public Health from 2010 to 2012, I found myself frequently and painfully at odds with current research and literally thousands of studies that proved to me that SDOHs will impact our lives in the most profound ways.
Yet I found the field and its most ardent practitioners lacking an explanation that showed the real power people have in controlling their personal outcomes. This is something that the public health field and my faculty sharply criticized by showing the medical model, which tells persons to control their health, has largely failed to promote wider population health metrics.
While I do embrace a “policy and systems” approach, I even more strongly believe that every person has the ability to make life-changing choices, every minute of every day—from the food they put in their mouth, to devices they watch daily, to the people they associate with, to the jobs they take or do not take (however awful often), to the way they manage their personal emotions. They have choices, and often they are cruel and brutally unfair choices, which often favor the privileged.
Frankl was famous for meeting with some patients, asking them to reflect on finding meaning in their lives over their entire life span, and providing the mental treatment they needed to take control of their lives without future interventions or drugs, which predominates the American model of mental health treatment. Some of his patients only required one session, and they could resolve to deal with life’s circumstances without any further intervention.
This is a radically and in fact dangerous model that challenges how the United States is grappling with mental illness nationally, though many practitioners use Frankl in their work. One psychiatrist I tweeted with wrote me back saying, “I’m far from the only one [using Frankl]! There’s a large humanistic community in the counselling/psychotherapy world.”
Frankl’s ideas continue to be studied, refuted, debated, and argued by learned and well-intentioned academics, which I think would amuse Frankl. He was more interested in the practical work of day-to-day living and less with becoming the subject of a cult following.
As one commentator I saw in a documentary who knew Frankl noted, Frankl was not interested in fame, otherwise he would be more famous today.
Paul Wong is one of many academics who have analyzed the ideas of logotherapy and mapped them in published work.
Here is just one example showing how theorists explain logotheraphy; see the table by Paul Wong on life fulfillment and having an ideal life.
Why Frankl’s thinking profoundly inspired me and thousands of others
For more than three decades, I have been wrestling with the concept of personal responsibility and the influence of our environment and systems that impact our destinies. Such factors include one’s family, country, religion, income, the ecosystem, our diet, and political and economic forces, among others.
I also have been fascinated by examples of people choosing hard paths in dire circumstances as the metaphor that defines successful individuals’ life narratives. In Frankl’s death camp reality, this ultimately boiled down to choosing to be good, and helping fellow prisoners, or choosing to partake in evil, which many prisoners did as brutal prisoner guards called kapos.
No one gets a free pass in this model, and all people in all groups can be one or the other, Frankl says. “In the concentration camps, for example, in this living laboratory and on this testing ground, we watched and witnessed some of our comrades behave like swine while others behaved like saints,” writes Frankl. “Man has both potentialities within himself; which one is actualized depends on decisions but not on conditions.”
I had not been able to order these two lines of thinking into a coherent set of principles, as Frankl so perfectly did. When I stumbled on him quite by accident or maybe design this summer, while reading books by Robert Greene and even management guru Stephen Covey, I had that most rewarding and delicious feeling of “aha.” It was more like, “Wow, what the hell was that!”
It felt like a thunderclap. I almost reeled from the sensation. I then began to tell every single person I know about Frankl, and I learned many of my colleagues had already read him. I felt robbed not one teacher or academic, at three respected universities I attended, had covered or even mentioned Frankl, when his ideas are foundational to our understanding of the fields of psychology, public health, business, organizational behavior, religion, and the humanities in the 21st century.
Frankl deserves vastly more attention then he is given by health, mental health, and social activist thinkers. That is a shame too, because as a speaker, Frankl brimmed with enthusiasm and could convey complex ideas in the simplest ways to reach his audience. Watch his presentation at the University of Toronto–a brilliant performance.
Frankl’s ideas matter to each of us, in everyday life
Photo courtesy of PBS, showing a pensive and thoughtful Viktor Frankl. Click on the photo for a link to the web site.
One my most satisfying feelings is discovering that one’s personal life experiences and ideas on issues as big as the meaning of life also resonate profoundly with millions of others—those who have read his work. Even more gratifying is discovering that the core principles to living life amid hard choices can be grounded in principles that can help everyone, even in the most dire of personal experiences.
My own travels in the developing world stand out for me. I met countless people facing vastly more painful, difficult, challenging lives than I have faced. Yet, the wonderful people I met had nothing but smiles and treated me with genuine sincerity. I had to ask myself, why is it that so many people are clearly content when their surroundings indicate they should be experiencing utter despair and even violent rage. Why is there kindness in their hearts and peace with their reality.
These young men, all Copts, a persecuted minority, highlight for me the depth of goodness one finds in the world, even when many have no material foundation that suggests they should be happy.
I understood at all levels what I was experiencing. But Frankl’s framework ties this rich set of personal experiences to all of us, and to larger existential ideas of what we are meant to do with our time.
For Frankl, the answer is just doing what life needs us to do. As Frankl wrote nearly 70 years ago, “Life ultimately means taking responsibility to find the right answer to its problems and to fulfill the task which it constantly sets for each individual.”
With that point, I now must ask you, the reader, What are you doing with your life, and are you doing what you are being asked to do? You cannot escape this question, and if you avoid it, you will always have the pain and emptiness of not listening to your own calling. The choice of course is your own.
Public health, as a profession and system to improve population health, continues to fall short in the United States.
Since the start of the Great Recession, nearly a quarter of all employees working for local health jurisdictions have been downsized or laid off because of funding cuts to already meager budgets. The National Association of County and City Health Officials pegs the attrition at nearly 44,000 workers–a fact reported on this blog before.
Proportional changes in inflation adjusted spending for public health (CDC) versus health care spending in the United States.
Today, most Americans have little idea what public health does, why it matters, and why its funding is critical to improving health outcomes at the population level. For that matter, half of all Americans cannot even identify what the core elements of health insurance plans are.
From its start as a profession in the United States in the early 1900s, public health was deemed to have a political-activist function. In fact, noted public health pioneer C.E.A. Winslow, Yale’s first chair of public health, promoted universal medical care in the 1920s as a principle of sound public health policy, backed later by other public health practitioners in the next two decades who unsuccessfully called for a form of universal health care.
Winslow’s often-quoted definition of public health called for the “development of the social machinery which will insure to every individual in the community a standard of living adequate for the maintenance of health.” Such efforts were overt and unashamed calls for political action and advocacy, the likes of which are mostly not heard today from the profession.
10 essential public health services: a recipe for political impotence?
Since 1994, the U.S. Centers of Disease Control has pushed the “10 essential public health services” model as the gold standard for defining public health’s realm of practice. As far back as 1999, the CDC claimed, “The overall goal for public health’s infrastructure is to have every health department fully prepared with capacity to fulfill the Ten Essential Public Health Services and every community better protected by an efficacious public health system.”
The 10 essential public health services is the U.S. model, not a global model, for defining the public health profession’s realm of practice.
This model has rippled outward to every public health agency, every school of public health, and all professionals in the field as the benchmark to measure quality and effectiveness. Logic models have been developed to see how well health departments were doing according to this standard. Anyone who works in the field is told that these services define who we are and what we do.
All the while, public health budgets have been slashed nationally, and at the state and local level, workers have fled or were pushed out of the profession. Still the field of public health continues to push its competent but still toothless model for what is considered a best practice—the 10 essential services.
While evidence-based and certainly valid, this 10-step model is also a self-defeating set of quasi-religious commandments that fails to address the harsh political realities related to developing legislation and orchestrating fights over budget appropriations. It also fails to call for advocacy and political activity, which can and have pushed public health efforts far greater than these prescribed activities.
Politics, money, and real power
For-profit entities working in the health sector thrive because advocacy and political engagement are fundamental to their business models and bottom lines, unlike the model of inefficacy promoted for the public health profession.
For instance, pharmaceutical powerhouse Pfizer unabashedly states, “We believe that public policy engagement is an important and appropriate role for companies in open societies, when conducted in a legal and transparent manner. … The Pfizer Political Action Committee makes contributions to candidates for federal office, and fully discloses its contributions on a regular basis to the Federal Election Commission.”
Pfizer, the multinational pharmaceutical firm, published its political spending activities in the United States for the first half of 2013.
While for-profit health interests march forward, with ever more dollars and clout, public health continues to retreat. The President’s budget request in 2014 for the CDC, the agency charged with protecting America’s health, is a measly $6.6 billion (for its program level expenditures)—a drop of $270 million over 2012.
This dip likely reflects pushback by GOP lawmakers in the current Congress, who view CDC’s public health activities as synonymous with overt advocacy. Language in funding measures, in the current session of Congress, has attempted to limit federal dollars for grassroots efforts by public health practitioners to lobby on behalf of specific legislation, particularly on efforts to address chronic disease and obesity.
Generally, public health advocacy is not lobbying, which is prohibited when it involves federal or earmarked funds. Exceptions include study or research and discussions of broad social problems.
So it is not surprising that government-funded public health bodies have been generally shy, and in the case of firearms legislation, nearly totally muzzled, from discussing firearms deaths since congressional language banned funding of firearms research starting in 1996. (In my opinion there has been a failure of leadership in public health when such leadership was needed on the issue of firearms violence, which is a legitimate public health concern.)
But should bans on using public funds for lobbying mute the profession from pushing for advocacy approaches and political engagement?
Daniel Callahan and Bruce Jennings’ 2002 article in the American Journal of Public Health examined the ethics of public health advocacy. They noted, “Politics is a necessary component of public health, moreover, precisely in order to achieve public health policies and practices consistent with American traditions and values. Politics is the messy arena in which ultimate questions of the public good are worked out.”
Public health’s failures in the political mosh pit
A perfect example of what happens when public health was not fighting tooth and nail was President Obama’s Affordable Care Act of 2009, which ultimately squashed efforts for a single payer system—the long-held dream of public health advocates from the 20th century—and advanced a health insurance industry, market-based model for “health care” reform.
All told, advocacy groups in 2009 spent $3.47 billion for D.C.-based lobbyists to parse out issues, according to left-leaning Center for Responsive Politics. Not surprisingly, the lion’s share of that spending went to fight the health reform battle. Businesses and organizations that lobbied on “health reform” spent more than $1.2 billion on their overall advocacy efforts.
The good news is that this marked a jump of more than 300 percent from what APHA spent in 2012. It would appear that some in the field are waking up to the realities of fighting for public health where the most meaningful impacts can be achieved – through policy and legislation.
By comparison, just one big pharma company, Pfizer, spent more than $800,000 in the first six months of 2013, from local to congressional candidates and political parties nationwide (see chart above).
What is most discouraging is that future leaders entering the profession continue to be shortchanged by graduate programs that do not know how to prepare practitioners to win in the bruising political environment known as “upstream.” This is my general assessment of not just my graduate MPH program, but of the field that I still see through its obsessive and yet parochial obsession with the 10 essential public health services.
The CDC’s 10 essential public health services.
A very smart resource guide developed by the California Endowment sharply noted: “… many public health faculty do not possess the skills or experience to teach advocacy effectively. Faculty surveys show, for example, that despite advocacy for health being recognized as an ethical responsibility and required competency of health educators, many health education faculty do not see themselves as competent for teaching advocacy and lack instructional materials to do so. Degree-granting programs in public health need to provide systematic training in social advocacy. In the absence of formal training in social change, public health graduates must learn this information and develop these skills on a catch-as-catch-can basis. Working in this way means that some will be less effective than they otherwise could be in advancing the health of the public.”
Thanks to everyone who has taken time to visit my blog focussing, mostly, on public health and health. I continue examining issues with the additional perspectives of history, culture, personal experience, and enterprise journalism. This month I crossed the 20,000-views threshold. See the screen snapshot below, taken today.
WordPress’s outstanding analytics tools provide a snapshot how many visitors and views have been recorded, in November 2013, and since I launched this blog in late March 2012.
WordPress’s analytics also report the following categories and tags attracted the most eyeballs:
Tags & Commentaries: Most popular topics you’ve written about
Topic & Views
Public Health 81
Health 77
Travel 57
Obesity, Sweden, Sweden, most beautiful women, Sweden has the world’s most beautiful women, infant mortality, life expectancy, Norway, Nordic Countries, public health systems, national public health investments, beauty stereotypes, national stereotypes, national obesity rankings, fat countries, obesity health threats 51
Photography 18
Native American 12
Africa 11
Human Rights 10
History 10
The most popular post on my blog looks at why Swedes have a reputation for being attractive, and whether that is related to the country’s strong public health system and universal health care. No doubt a fair number of visitors came looking for pictures of blonde Swedes in bikinis, but hopefully came away with some knowledge of how investing in health upstream can pay dividends that are linked to, yes, physical appearance and overall health.
The data are great validation for the idea that first launched this enterprise. It began during a spirited discussion at the University of Washington School of Public Health about the value and validity of training future public health leaders to specialize in publishing in peer-reviewed journals as opposed to open-source communications like WordPress-enabled blogs or social media or non-scientific publications. This is a topic that is being debated by many seeking to improve public health’s relevance for the year 2013 and beyond.
Having public relevancy in the face of funding cuts remains a critical issue in the field of public health, which has seen its workforce at the local level shrink by 44,000 jobs, or nearly a quarter of all workers, since the start of the Great Recession. Budgets in local health jurisdictions have been slashed to the bone according to a national survey of those organizations by the National Association of County & City Health Officials (NACCHO).
In fact, I would recommend to anyone contemplating a career in public health, outside of epidemiology or biostatistics, to consider advanced degrees in law, business, or applied health like nursing rather than this field, based on the national employment data. Or future public health leaders can learn through other means how to integrate new tools of communications to engage the public with research, to build support for funding health.
In fact, those who now manage the nation’s graduate public health programs need to use the tools of program evaluation, which they teach in the nation’s finest universities, and engage in a serious discussion if their education model is still working and achieving longer-term goals and ultimately leading to a better public health system and healthier country.
How many MPH graduates in 2013 found jobs within six months? Is that number acceptable? Why train a workforce for many jobs that may not be in high demand or nonexistent, with skills that are not reaching a wide audience, thus preventing the public from knowing what public health is and why it matters?
This will remain a fundamental issue at the heart of the crisis facing the field today and for years to come. Meanwhile, I think there will continue to be a bottoms-up response to how the profession adapts to change in the new era of diminished resources. I hope that this blog will continue to be involved in that larger discussion, and the numbers show that at least some online readers are hungry for information in easier-to-access ways.
On the first day in the new year, I read one of what will become thousands of similar stories that will be published this year in the United States about how firearms were involved in completely senseless and preventable violence.
To understand why the United States has so many shootings, one may wish to buy this book, Armed America: Portraits of Gun Owners in Their Homes, by Kyle Cassidy. Go to http://www.armedamerica.org/. This book cover photo offers one perspective on the national crisis over the nation’s gun-related violence.
In this particular instance, a 54-year-old woman reportedly shot a 24-year-old man in the thigh over a dispute that he was shooting fireworks at her property in rural Lake Stevens, Wash. No, I am not making this up.
While no one died in this New Year’s eve confrontation, the story barely received three paragraphs of news coverage, as it lacked the dramatic horror that the media exploit when mass homicides occur involving often-legally purchased weapons. There were no dead children or mentally deranged men in military gear loaded with weaponry. Were this story to occur in Canada, or say Japan, it would have received much different coverage.
While we may assume this seemingly “bland” shooting will be counted in national data, that is not guaranteed. It likely could be ignored.
In response to uncertainty over national data, Slate Magazine, on Jan. 1, 2013, published a story called How Many People Have Been Killed by Guns Since Newtown?. The article alleges guns statistics are “surprisingly hard to come by.” Slate claims it will track the toll of gun related killings with an an anonymous publisher with the Twitter feed @GunsDeath to create an interactive tracking feature. The articles asks readers who know about gun deaths in their community that are not counted on its interactive map to tweet @GunDeaths with a citation, and it will be added to the feed.
The Brady Center keeps a daily tab on gun violence–go to the right corner of the center’s home page for the shooting count, based on CDC data.
The Brady Center, the best known nonprofit that is working to pass legislative fixes to issues such as the sale of semi-automatic weapons and closing loopholes that allow for guns sales without background checks, uses data from the Centers for Disease Control (CDC) (2008-09 estimates). It then makes an estimate of the number of killings a day that may not correspond to the most recent trends. The source data is captured by the CDC National Center for Injury Prevention and Control, reported and accessible through the web-based Injury Statistics Query and Reporting System.
A lesson in how to silence public health researchers, and yes it is about the money
Slate’s professed shock at the lack of poor tracking of gun-related fatalities should actually surprise no one who has monitored the muzzling of research on gun-related violence since the 1990s by the National Rifle Association (NRA), the gun industry’s lobby, and its allies in Congress.
According to a newly published article by Dr. Arthur L. Kellermann and Dr. Frederick P. Rivara (both of whom have MPH degrees), in the Dec. 21, 2012, edition of the Journal of the American Medical Association, gun research at research universities that is funded by the federal government has been systematically quieted by pro-gun forces since a ban was enacted on the CDC in 1996, mainly through budget language. Pulling funding, in effect, silenced the nation’s public health agency on a critical public health issue.
The budget language, which remains in effect today, stated “none of the funds made available for injury prevention and control at the Centers for Disease Control and Prevention may be used to advocate or promote gun control.” While it is not clear why individual CDC officials or even highly paid medical and public health professionals have not more publicly risked their professional standing to challenge this language, the authors of the study note, “Extramural support for firearm injury prevention research quickly dried up. Even today, 17 years after this legislative action, the CDC’s website lacks specific links to information about preventing firearm-related violence.”
Rivara and Kellermann further state that the language restricting such research was expanded after a 2009 study that was federally funded, this time by the National Institute on Alcohol Abuse and Alcoholism, if a gun increases or reduces the risk of firearm assault. Congress, in 2011, during the Obama administration and amid the Tea Party insurgency of 2010, “extended the restrictive language it had previously applied to the CDC to all Department of Health and Human Services agencies, including the National Institutes of Health.”
The two authors highlight other efforts taking place national to stifle medical professionals from speaking out, such as Florida’s law (HB 155), which put health care practitioners at risk of penalties, including the loss of their licenses, “‘if they discuss or record information about firearm safety that a medical board later determines was not ‘relevant’ or was ‘unnecessarily harassing.'”
How silencing plays out at research universities, quietly and likely without intent
This blog has reported that the silence within the research community can be found at major public health research programs, such as the University of Washington School of Public Health, which I attended from 2010 to 2012. I was unable to find any faculty actively teaching future public health leaders–my classmates–about firearms safety research or gun violence in the school’s public health curricula.
It should be noted Dr. Rivara is an adjunct faculty member of the UW School of Public Health, and Dr. Kellermann and he are also graduates of the same school (for their MPH degrees). Dr. Kellerman was in fact my graduation commencement speaker, and proved to be a passionate scientist and advocate to all of us. However, my review of courses did not reveal any classes focussing on gun violence as a public health issue; this does not mean Dr. Rivara and other faculty did not cover this topic in their classes. (It should also be noted that a keyword search for “guns” on the UW SPH web site today, Jan. 2, 2013, yielded only three pages, one focussing on Dr. Rivara and another focussing on Dr. Kellerman.)
During my studies there, I repeatedly raised this anomaly to my professors and during seminars in front of as many faculty as possible–often to the point of becoming an annoyance to those who had heard me ask the same questions repeatedly. But short of actually sitting in on faculty strategy sessions or having any survey data, it is impossible for me to know the reasons why my former school choose not to include this topic in its curricula. There were and remain classes on issues that do receive federal funding: tobacco cessation, obesity and nutrition, maternal and child health, and much more. All are worthy topics, but these were the winners, guns was a loser.
My guess remains it was purely a matter of funding, or lack of funding, and the intense internal pressure on junior faculty to pursue research dollars highly coveted by all departments that were not tied to this pariah topic. Thus the silencing of research continued, without any alarm bells raised from a larger community of researchers, who should be the most active and who should have been leaders, locally and nationally. That is how it works.
Dr. Rivara’s primary role is as a faculty member at the UW School of Medicine, Department of Pediatrics. To his credit, he has shown continued national leadership on gun violence. He and Dr. Kellerman deserve great praise for their lifelong service and work on this topic. Hopefully their article also will shame and embarrass their distinguished academic peers–locally and nationally–into either creating endowed teaching positions or a campaign drive to fund research that can shed light on this national public health crisis that has seized the nation’s attention since the massacre of 20 children and six faculty in a public school in Newtown, Conn. in December. MPH students also can lobby for change too, despite the hazards of confronting faculty who grade and often employ them as assistants.
Given that many faculty at these institutions can earn salaries well above $200,000 annually, some may be reluctant to jeopardize their professional careers or positions in the name of public-minded research on a topic that is at the center of one of the nation’s greatest moral debates since the Civil Rights movement and perhaps since the violent ending of slavery during the Civil War.
Gun researchers who have not been silenced by budget threats
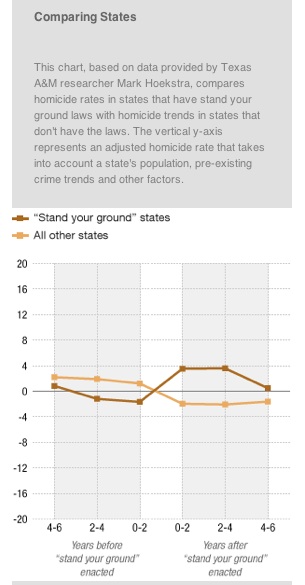
Researchers not blocked by the ban on the CDC and NIH have shown that a prized policy goal of the NRA and gun makers, expanding “standing your ground laws,” have lead to more homicides.Researchers have found that states with a stand your ground law record more homicides than states without such laws.
Data from the study by Hoekstra and Cheng, as published on the NPR.org web site (Jan. 2, 2013).
Two economics researchers at Texas A&M University, Mark Hoekstra and Cheng Cheng, found that the laws “do not deter burglary, robbery, or aggravated assault. In contrast, they lead to a statistically significant 8 percent net increase in the number of reported murders and non-negligent manslaughters.” The findings run counter to the argument of the primary proponent of such legislation, the NRA.
On average, there are about 500-700 more homicides a year among the 23 states with stand your ground laws because of these laws: “One possibility for the increase in homicide is that perhaps [in cases where] there would have been a fistfight … now, because of stand your ground laws, it’s possible that those escalate into something much more violent and lethal,” says Hoekstra.
On Sept. 19, my University of Washington graduate student health insurance plan expires. I paid $607 a quarter last year, four quarters a year, for two years for this plan. It was OK. I never really “used” it for anything. I did have my knee looked at, and a finger was inspected once that got dislocated that I actually fixed, but no real “medical care” was ever provided except consultation. Only one visit really required a specialist’s expert analysis, but I actually deduced a similar conclusion from online research. Short of a medical test, even that expert opinion was just that, an opinion. So I am left wondering what this investment served. It did not cover in-house physical therapy, massage, or chiropractic care—all forms of medical care that I truly believe promote health and wellness without expensive, harmful pharmaceuticals and that use non-invasive techniques to promote healing through touch and manipulation of the body’s muscles and skeletal system.
Massage should be covered at higher levels by all insurance plans, as it provides excellent health outcomes with few negative effects and no medication.
I was supposed to cover those expenses “out of network” at 60%. As a former graduate student, I had to weigh medical care versus, well, paying for food and rent, and I simply put off the care I needed the most and used to get when I had a plan with my former employer in Alaska – chiropractic care and massage therapy. There were times I was in excruciating pain that simply had to be ignored because my insurance did not cover it, and those problems could have been addressed if I paid for much of it, after my deductible.
So now I am in the open market of insurance again. This is that wonderful place where the “invisible hand” of Adam Smith is supposed to provide solutions without “government interference.” Well that is not the case. The market is somewhat regulated by the Washington State Insurance Commissioner. They put together a good web site to help consumers understand the nine companies that offer health insurance plans in this state and the types of plans available to them. I think they did a good job.
Such communication for consumers is critical, as insurance companies prefer to communicate in “insurance speak” language involving legalese and jargon such as “co-pays,” “deductibles,” and let’s not forget “pre-existing conditions.” Here’s just a taste of one clause from one plan on how they try to limit coverage for a “pre-existing condition”: “Pre-existing conditions: these plans contain a nine-month pre-existing condition clause that excludes coverage for any condition for which there has been diagnosis, treatment (including prescribed drugs), or medical advice within the six-month period prior to the effective date of coverage, for which a prudent person would have sought advice or treatment. Section 6 of the application for our individual and family plans will help us determine whether you have creditable coverage, which would allow [COMPANY NAME REMOVED BY AUTHOR] to waive pre-existing conditions/exclusions for you and/or your dependent(s).”
No, choosing insurance is never easy because the language is often confusing and many non-experts cannot decipher the fine print of the brochures with happy, smiling people used to lure in customers.
Such language is not simple or easy to understand, and in theory, the Patient Protection and Affordability Care Act (health insurance reform passed by Congress recently) will make it impossible for insurance companies to deny persons health insurance in the future because of a pre-existing condition. It is not clear if non-English speakers can understand this information at all. While many people have fought with insurance companies, many lower-income or less-educated persons may not have significant experience navigating complex legal documents that, quite frankly, I think people with MBAs or law degrees do not fully understand. Here are two companies’ plans that offer health insurance to individuals in the state of Washington (there are exactly nine corporate players in this limited market): LifeWise, Group Health.
I chose LifeWise. I am waiting for them to approve my plan. I will have to have proven I actually had coverage before (I did as my UW plan was owned by them) and am likely not a deadbeat. I am sure they are probing my legal, credit, even personal records as I write this to determine if I have been an actuarial risk to providers, if I have some terrible health condition that would harm their profit margins, and if I am generally on the up and up as a possible customer to help them make a “reasonable rate of return,” which is really all a company can hope to do. This all is, of course, unlike other developed democracies, because our country continues to refuse to adopt a single payer plan that other countries like Canada and France have taken up with better population health outcomes for their citizens and less gauging of consumers.
So what will I get if I am approved? I signed up for the basic catastrophic plan called “Wise Simplicity”. I would pay $160 month as a nonsmoker, and have a $10,000 deductible (compared to an $1,880 deductible that would cost me about $370 a month). So if I am hit by a car, I pick up the first $10,000 out of pocket? Great, eh?
So what do I get with the barebones plan? Well, basically a plan that tells me not to get sick and certainly don’t have an accident that costs $9,999.
I simply cannot afford another plan now. And this deeply worries me, until I get a job with coverage (and that is coming soon – yeah!). Two people I know in my immediate circle of friends just had enormous medical bills. One friend had elective knee replacement surgery. I cannot imagine that is less than $50,000 to $100,000 in costs (surgeon, anesthesiologist, several nurses, equipment, rehab, etc.). Another friend had a horrible and likely allergic reaction to a standard immunization and developed a syndrome that sent them to the hospital, where the same issue ensued with specialists, etc. My friend guessed the bills before insurance will be at least $100,000. So as I bike down Seattle’s dangerous roads, avoiding cars that do not know I am there as the driver texts a message about whatever, I contemplate just how flimsy my health care coverage really will be come Sept. 20. I guess the answer is what some running for office suggest – just don’t get sick. You know what I really do not have a choice. Adam Smith’s invisible hand I guess is making that possible, but why do I feel more like the hand is choking off my air supply and giving me a sucker punch when I am not looking.
Like many people in the United States and around the world, I was horrified by the news on July 20, of yet another mass murder in the United States involving firearms. We still do not know as I write this post the motives of the alleged suspect, a 24-year-old medical student named James Holmes. Nor do we know yet how he acquired the multiple firearms—a semi-automatic rifle, a shotgun, and a pistol, according to initial reports—used to kill 12 people and leave 59 wounded. Press reports quote police officials saying he bought his firearms legally along with 6,000 rounds of ammunition. We do know that neither President Barack Obama or GOP presumptive contender Gov. Mitt Romney uttered the word “gun” in their public comments the day after the mass murders.
Alleged mass murderer James Holmes in a photo published by many media sources.
For his part, New York City Mayor Michael Bloomberg, a billionaire who does not have to worry about his political career even if he is voted out of office and who can afford to defy special interest groups because of his great personal wealth, was quick to criticize both presidential candidates for failing to put forward plans to address gun violence, which is a concern of many elected officials in any sized city. “Soothing words are nice,” said Bloomberg, “But maybe it’s time the two people who want to be president of the United States stand up and tell us what they’re going to do about it, because this is obviously a problem across the country.”
Boston Globe columnist Derrick Z. Jackson wrote on July 21: “Gun control has so completely disappeared from debate that John Rosenthal, founder of the Newton-based Stop Handgun Violence, told me this week before the Aurora shootings: ‘I’ve never seen more spineless cowardice and lack of national leadership. Can you imagine the outrage if instead, 83 Americans a day died from hamburgers?’ Instead the conservative Supreme Court struck down urban handgun bans. Last year saw record gun sales in America, based on FBI background checks, as the gun lobby whips up utterly false fears about Obama taking people’s guns away.”
Such mass killings like we saw in Aurora, Co., now occur with alarming frequency in the United State. Where I live, Seattle, we have experienced a wave of mass shootings during the last two months, the most lethal at a University District area restaurant called Café Racer and elsewhere in the city on May 30, that left six dead, including the alleged gunman.
From a purely statistical perspective, firearm violence is a national health issue, if not a crisis. The Centers for Disease Control and Prevention (CDC) reports that the number of firearm homicides in 2010 in the United States was a whopping 11,493, or 3.7 deaths per 100,000. And the role of firearms in suicides was nearly twice that rate. The CDC for 2010 attributes firearms in the suicides of 18,735 persons in the country, or a rate of 6.1 per 100,000. All told firearms are linked to 30,228 deaths annually at last count. This is a truly staggering figure, and one that should have the entire medical and public health community demanding that moral and political leaders in this country develop a broad array of interventions to reduce these numbers, the way we mobilize yearly to dress in pink and run against breast cancer or embrace other campaigns designed to save lives and promote health. By contrast, Japan counted 11 homicides related to firearms in 2008, or a rate of 0.0 per 100,000 in epidemiological terms.
So why is the medical and public health community silent? Well, the answer is simple. It is about politics and money. Specifically, it is about the lack of federal money. And of course those who should be out front on this issue, including heads of hospitals and medical associations as well as faculty and heads of health sciences universities, are not demonstrating the needed moral courage to speak truth to the supporters of the NRA, business interests, and political groups, who exploit American fears about government and who seek to maintain the status quo politically through fear-mongering. That job is mainly falling to journalists and citizens groups mostly, as well as victims of crimes and their families.
The Nieman Foundation at Harvard University reported in February 2012 that the gun industry’s main lobbying arm, the National Rifle Association (NRA), has “systematically suppressed data about gun violence and the impact it has on Americans’ lives.” The CDC in the early 1990s was releasing studies that found that guns in the home presented a greater danger to the occupants than potential home invaders. In response the NRA helped to prevent the funding of research on firearms’ death and injury. As a result, reports the foundation, the CDC appropriations bill the last 15 years has contained this language: “None of the funds made available for injury prevention and control at the Centers for Disease Control and Prevention may be used to advocate or promote gun control.” And this year, the NRA successfully added a similar amendment to the National Institutes of Health (NIH) appropriations language.
The most well-known advocacy group that promotes strict gun regulation, the Brady Campaign to Prevent Gun Violence, was extremely critical of the CDC in 2011 for, in its words, requiring researchers financed by the CDC to give the CDC a “head’s up” when they prepare to publish firearms-related research. The CDC, in turns, shares that information with the NRA as a courtesy. “If the CDC is allowing the NRA to review its studies, it’s a deeply troubling practice,” said Brady Center President Paul Helmke. “To have a government agency open itself and its science to the influence of any interest group, particularly one whose policies undermine the safety of our families and communities, is improper, offensive, and unjustifiable. We need science that we can trust.”
One has to look no further than the Department of Health and Human Services’ (DHSS) exhaustive annual report called Health, United States, 2011. It lists the word firearms just nine times, and buries firearms data deep into the report, making that information effectively unimportant in the overall health assessment for the country. Meanwhile the introduction to that report profiles motor vehicle deaths (about 40,000 deaths annually) and does not profile death by firearms (suicide or homicide, which number more than 30,000 annually). One has to wonder how connected the funding ban is to this type of editorial decision by the DHSS and the CDC, which publish this document.
Of course many proponents of very limited gun control disagree firearms-related violence is a “health” issue. One pro gun blog, published by a group called AmmoLand.com, calls those who would choose to address firearms safety “elite gun banners.” (The those being criticized is the CDC.)
Which item does the CDC and many public health research universities consider more of a public health threat, and which receives more research dollars and scholarly attention?
What we are seeing, at least at public health departments through funding mechanisms, is a full-court press on chronic disease linked to unhealthy food like, oh fatty french fries. When it comes to clogged arteries but not loaded semi-automatic weapons, the CDC doles out millions dollars ($103 million at last count) through Community Transformation Grants. It continually baffles me how trained scientists who work in health care flat out follow the money to pursue research grants to get more people to eat fruits and vegetables and stop smoking while keeping mostly silent as people in their communities are gunning themselves down and others.
I never understood this during my studies at the University of Washington School of Public Health, where there is not one course where firearms issues are addressed as a public health priority, at least according to my understanding of the courses offered. I did a quick search on the UW SPH web site on July 21 and found just seven references to firearms, six to guns, and 233 references to obesity. (UW researchers were involved in a joint study published in 2012 about gun storage cabinets in Alaska, but one would expect more given the numbers.) But this is no different than at any publicly funded health research university that relies on large federal grants to sustain its faculty and facilities. Clearly this impacts what future public health leaders are taught. During my two years in my program at the UW SPH, which used problem-based learning and cases that touched on everything from obesity to smoking to HIV/AIDs to homelessness to influenza, our classes never discussed firearms violence as a public health concern. (Note, that changed this year for the class behind me thanks to comments raised by my cohort to faculty for suggesting new topics).
In my frustration today, I even wrote to my member in the U.S. House of Representatives, Dr. Jim McDermott, by clicking the on the topical area of “gun control” to submit my email to his staff. I know from past experience that federal lawmakers never read 99% of such emails, and their replies usually do not address the contents of constituent communications, instead relying on general policy statements that amount to little substance. Still, I felt compelled to express my continued disappointment at the failure of leadership that he and others are demonstrating on this health and policy issue:
“As a public health professional and as your constituent, I am writing today to ask if you can inform your constituents what you and your allies, including in the health community and law enforcement community, are planning to do in terms of a meaningful policy response to address the proliferation of firearms and in terms of providing funding to health professionals to begin to address this issue as a legitimate threat to the health of U.S. citizens? Can you provide any details about how you are working locally with groups seeking to have upstream and federal actions to begin to chip away at the powerful special interest groups that have hijacked the public debate on firearms? Are you seeking to challenge blue dog Democrats or Republicans who continue to communicate talking points that equate the Second Amendment of the Constitution with the sale of personal weapons that in no way correspond to the wording or intent of the Constitution or the intent of the framers of the Constitution? I await your leadership. If there is to be no action, than one wonders why there continues to be cynicism of citizenry about the leaders we elect to Washington to do the people’s business, not the business of special interests that are allowing weapons manufacturers to profit from the misery of innocent citizens wiped out by a completely controllable problem, were there true courage and leadership to face down the attack ads. People can lead, but well, so can the leaders we elect. I await to hear your strong voice.”
Before I am cut off from the University of Washington’s online library services as a former tuition-paying student (very expensive), I am researching and downloading articles on public health and health issues that I will no longer be able to access without paying exorbitant fees to companies like Netherlands-based Elsevier. Such companies are making a killing selling peer-reviewed articles at high prices, so only fee-paying institutions can access the research that is funded by public dollars.
Elsevier sets a not-too-cheap price for the public to “buy” peer-reviewed articles, often funded by public money and taxpayers.
According to an April 24 article in The Guardian, more than 10,000 academics are already boycotting Elsevier, to protest its business model that sets high prices for peer-reviewed journal articles and access to them. This protest has been dubbed the “cost of knowledge.” The Guardian reports that many university libraries pay more than half of their journal budgets to the big boys of academic publishing, which also includes Springer and Wiley.
One optimistic comment from the editor-in-chief of the prestigious scientific journal Nature notes open access to scientific research articles will “happen in the long run.” Well, I sure hope that happens, but I may not bet on it.
In fact there is a display about this debate in the UW Health Sciences Library (my home away from home for the last two years) on the economics and ethics of charging for scientific articles that publish research funded by taxpayers. Right now, only those who pay fees can download many of these journal articles at such university research libraries like this one. And it is through peer-reviewed articles that academics get tenure, validation, and grant funding and that research enters into the realm greater scientific discourse, and eventually the realm of policy-making and responses by the private sector.
The Guardian reports that prestigious Harvard University prepared a memo to its 2,100 teaching and research staff calling for action, claiming the institution could no longer afford price hikes imposed by the aforementioned publishers. These fees, in effect, are paid by students like me.
I paid nearly $45,000 in tuition and fees to the University of Washington for two years of study, and during that time, tuition was hiked 10% each year in my school, the School of Public Health (the last hike just being approved by the UW Board of Regents the first week of June). So the business model of these publishers is definitely one driver in uncontrolled tuition inflation that is putting an entire generation of graduate students into unsustainable debt. Even the very conservative UW Board of Regents, in their announcement of another round of tuition hikes for undergraduate students, issued a formal declaration expressing “concern for the sustainability of Washington public higher education.”
In my last week of classes at the University of Washington, I partook in a discussion on this topic and shared my concern with a UW School of Public Health faculty member that public health students are being trained to write and publish scholarly articles, many of which may never be published in open sources outside of subscription services like Elsevier. One suggestion I offered was to help prepare the next generations of graduates to help communicate the science and research findings of their field for open-access sources. The Centers for Disease Control and Prevention already does this in its publications (the Morbidity and Mortality Weekly Report), and does this well, but more needs to be done by future public health practitioners if a sustainable model can be developed to pay for the research to reach the public via open source platforms.
My bet is the next generation of public health influencers, like my colleague Valerie Pacino, will be blogging as much as they are writing peer-reviewed articles, and having an impact doing it.
On May 11, 2012, faculty and students gathered at the Center for Urban Horticulture to celebrate accomplishments achieved during the academic year. Such events are important, I think, particularly when those honored truly deserve the accolades of their peers. To my delight, three graduate students who I know and respect greatly won top honors from their respective departments and programs, and even the entire school: Valerie Pacino, Bridget Igoe, and Mateo Banegas. It was awesome to see this kind of recognition of people who I am confident will be leaders in whatever place in health care, policy, science, or research they find themselves. It is so fun to get to meet people who you know will be making their mark in the world.
As for me, I am just delighted to be at the end of the long, expensive, and interesting journey. At times exhausting, and at times fascinating, graduate programs no matter what the field or the school have their ebbs and flows. The best part of course is when you reach the end and look back on all you have done. To celebrate the final class of my program (Community Oriented Public Health Practice), one of my classmates surprised us all by preparing mimosas before noon, while we did a very thorough review of management and organizational behavior theory (and I really enjoyed this block, taught by Professor William Dowling). I still have a couple of presentations to make, and of course get that all elusive great job doing what I love to do, but all in due time.
Rudy Owens, final day of coursework at the UW School of Public Health, turning to the heavens in thanks at Seattle’s Discovery Park (May 17, 2012).
On March 27, 2012, I submitted my capstone research project for my master of public health program at the University of Washington School of Public Health (UW SPH). (My program is called Community Oriented Public Health Practice.) My research focusses on the effectiveness of Seattle emergency preparedness communications, what residents know about emergency preparedness, who they trust, and how well these outreach efforts are reaching vulnerable residents. I really enjoyed this project and enjoyed the many professional relationships I developed during the course of my research. I also greatly enjoyed sharing my research findings with the emergency preparedness community of greater King County on Feb. 16, 2012.
From what I was told, my research project was the earliest any project had been submitted ever (a full quarter early) to COPHP. And it was a project well received by the City of Seattle, with whom I worked and who have already published my reports to them on their web site (look for SNAP Research – “Owens Report 1” and “Owens Report 2” at www.seattle.gov/emergency/publications/#s). I also have published copies of nearly all of my original research and papers submitted to the UW SPH. You can review and download my finished work.
However, being early means you can’t celebrate. It is “out of place,” as some rituals are tied closely to shared experiences, not individual ones. At my undergraduate school, Reed College, the culmination of the undergraduate thesis (required for all students) was a thesis thermometer in the hallway of the main administrative building that marked every thesis turned in. The ritual culminated in a massive parade and a fun weekend called Renn Fayre. I always thought the thesis was a somewhat onerous burden with little practical real-world applications (for me at least), but at least the school “got it” when it came to marking the end of a long and arduous journey in academia. I have my own ritual in mind for when I get my next diploma. It will be very very fun. I’ll do it somewhere in the woods, and I look forward to that event.