One thing I have never shaken since my days as a rookie reporter is my penchant for calling out the obvious. This is one of the sacred duties of the press: to speak truth to power. This also means calling a spade a spade, and bullshit for what it is, and what it smells like.
Anyone who has ever worked in the business of reporting news and telling facts knows this is one of the press’s sacred trusts—and myths—and the clearer we are in doing that, the better our society is from having that unbiased information.

Today, I stumbled on Marcy Wheeler’s blog, the Empty Wheel, which tackles many hot-button policy issues. Last year she blogged about climate change in a piece called “The Cost of Bullshit: Climate Change, National Security, and Inaction.” She pointed out that the cost for maintaining the status quo was too high, even when major government agencies from the Department of Defense and the Department of State concluded that the issue was a critical concern to U.S. national interests. Yet, no actions were being taken by the government, and all of the reports on the emerging crisis were “mere bullshit—more wasted government employees’ time and taxpayer money.”
Sure easy for a blogger not on the payroll to diss hard-working public workers and policy-makers, right? Or, is Ms. Wheeler simply calling out the obvious, like reporters have always done, or thought they were doing.
Will a public health fad meaningfully address the main killers of Americans?
The cost of bullshit has been on my mind late, particularly regarding public health jargon that inflates busy-looking arm-waving, but does not change reality.
For me, one of the most frustrating aspects of working in the public health is the field’s faddish way it labels its collective actions to address chronic disease issues, such as obesity, using fancy sounding concepts like “policy, systems, and environmental change.” Mon dieu, what big words, what big ideas.
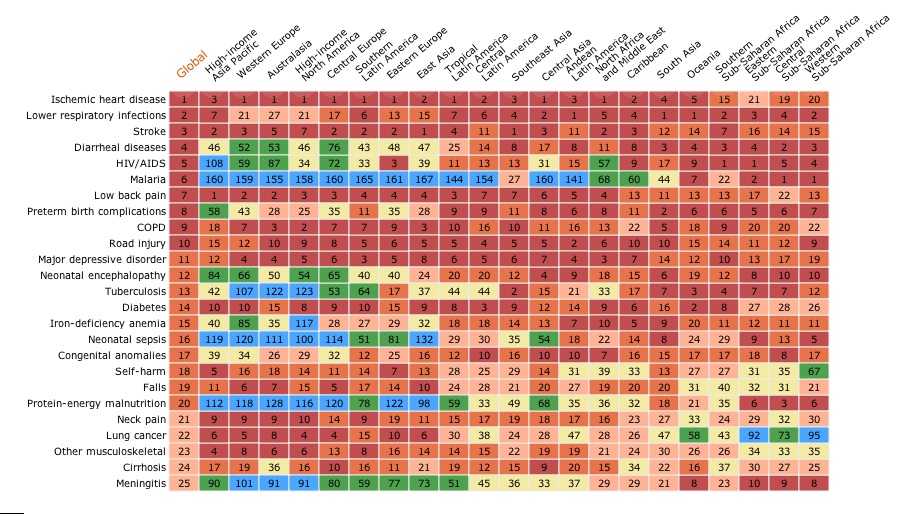
This is an expression coming from the top, from the venerable U.S. Centers and Disease Control (CDC), to explain national efforts to tackle the monster that is chronic disease—the leading causes of death in our ever-fattening and ever growing income-unequal country.
These diseases kill seven in 10 Americans, and of the CDC’s meager budget of under $7 billion for our national public health effort is a mere drop in the bucket compared to other priorities of the $1.2 trillion national budget that is so-called “non-discretionary spending.”

The CDC still estimates 18% of U.S. GDP spending is on healthcare, and a third of it at the place where the most outrageously overpriced and at the same time least effective primary care interventions can take place—hospitals.
So what do public health officials do, when faced with a handful of breadcrumbs thrown to them from Congress? They invent concepts that make it appear that public health is doing something, when there is little or no clear evidence population benefits are accruing based on investments at this level in the large ocean. Yes, I am talking about the catchy and jargon-laden ideas like “policy, systems, and environmental change.”
This is a hodge-podge of activities that encompass everything from starting farmers markets to promoting smoke-free buildings. Here are a couple of definitions I randomly found from some online sources:
- State of Mississippi: “Our environment and the policies and systems in it shape the pattern of our everyday lives and have a profound influence on our health. The design and walkability of communities, the availability of low-cost fruits and vegetables, and the smoking policies in our workplaces have a direct impact on our physical activity, diet and health.”
- State of Maryland: “Policy, systems, and environmental change (PSE change) refers to public health interventions that modify environments to provide healthy options and make healthy choices easy for everyone.”
- Fairfax County Virginia: “Policy, systems and environmental change is a way of modifying the environment to make healthy choices practical and available to all community members. By changing laws and shaping physical landscapes, a big impact can be made with little time and resources. By changing policies, systems and/or environments, communities can help tackle health issues like obesity, diabetes, cancer and other chronic diseases.”
Budgets for this kind of intervention exist in most public health jurisdictions, and public health leaders are doing to the talk, because they have so few funds to do the walk. But public health experts end up playing in a small sandbox when these investments are measured against other spending, and then we spend a lot of time trying to convince ourselves through published papers, webinars, conferences, and the like that this is working. The illusion is powerful, like the illusory power of the Iron Throne in the Game of Thrones, except the shadow from a fad still does not make meaningful change when the numbers are crunched and the costs are calculated regarding chronic disease.

Public health departments who get funding through competitive grants from the CDC spearhead these efforts and then spend extensive amounts of time documenting their work trying to prove the bread crumbs made a difference to the overall health crisis facing Americans.
About $200 million was doled out from 2011 and 2012 through an effort called Communities Putting Prevention to Work (the amount initially announced in 2010 was about $380 million). In one case, Public Health-Seattle & King County published findings that show its CPPW-grant-funded efforts in schools cut youth obesity in specific schools by 17 points. Great job, except the funding was not permanent and it was not renewed when the grant ran out. The program is now in the past tense.
In 2014, public health professionals learned another funding source, the Community Transformation Grants, which also promote the policy, systems, and environmental work, is being cut too. Some can argue the money is being allocated to other programs that tackle chronic disease, focusing on heart disease and diabetes.
More musical chairs without really changing the big picture again?
I do not mean to belittle the work of public health people doing this work. They are my colleagues. I respect them. And the work being done, like promoting activities to reduce tobacco use and get more people eating healthy food, should be continued.
But as a field, I am convinced this type of work is self-delusional because it hides the nasty realities of how much larger issues shape the public’s health, such as how transportation budgets are allocated, how cheap petro-based energy is spurring obesity in measurable ways, how legislation is crafted by special interests at the state and federal level, and how the principle of health care is considered a privilege not a right in the United States. (In Denmark, by contrast, the public funds about 85% of all health care through taxes, and the system is rooted in both law and a social contract that is premised on system where all citizens are provided free and equal access to quality health care.)

The nasty realities we do not want to think about, using a contemporary TV metaphor, would be what happens when the violent kings of Westeros cut deals and cut heads, to maintain order in that mythical, lovable place with White Walkers, a giant ice wall, and fire-breathing critters. Mother of Dragons, public health is not, that is for sure!
I imagine a new fad will emerge in public health in the next three years, like it does in management. We might change the concept, but we likely may even have a smaller piece of the government pies.
No, public health jurisdictions cannot stop working until we see changes on these fronts. But the more we in public health delude ourselves that we are making a difference with scraps from the table, the more easily we are duped into accepting that the larger model is as it should be, and how it shall always be.
We will continue kvetching about farmers markets and soda machines, but not moving in a rigorous way upstream, where budget deals are made with transportation dollars, for starters. And I think we have to start being honest with ourselves about what we are accomplishing in the sandbox and whether this is the best use of our meager and diminishing resources.