This newly updated sicence lab was left to the scrappers and criminals who have completely destroyed the school without any interference from the Detroit Public Schools.
The destruction at Crockett would likely be the source of public outrage in other U.S. cities, but not Detroit.
Scenes of devastation greet visitors to Crockett Technical High School in Detroit (taken September 2015).
(Click on each photo to see a larger picture on a separate picture page.)
A year ago, in September 2015, I visited my birth city, Detroit. I saw things I could not imagine were possible in the supposedly most powerful country in the world. I toured the city and observed impoverished neighborhoods, shuttered factories, empty homes in every corner of the community, and the omnipresent ruins from arson that have made the Motor City the arson capital of the United States. Detroit had a surreal feel. I called it City of the Future and published several photo essays and a photo gallery on my web site. The most memorable and heart-wrenching place I visited was the now shuttered Crockett Technical High School, at the corner of St. Cyril and Georgia Street.
The trashed and gutted Crockett Technical High School was listed for sale in September 2015 by the Detroit Public Schools, which failed in every sense to protect the school from destruction by scrappers and vandals.
In my last photo essay on this gutted and neglected facility of learning, I recounted that Detroit Public Schools (DPS) recently had implemented a painful round of massive school closures, carried out by DPS emergency manager Roy Roberts. In sum, 16 school buildings were closed permanently. In the previous decade, enrollment in the system had fallen 100,000 students, and by 2012-13, enrollment was about a third of what it was a decade earlier.
Death of a school by scrapping and bureaucratic negligence
What I learned during my visit to Crockett from two friendly neighbors who were across the street would have been intolerable in nearly any other major U.S. city. I wrote in my September 2015 photo essay, “They noted that the DPS police did nothing to stop the scrappers once the schools alarm system failed. First the scrappers busted the windows and ripped out the metal. Then they went to work on the interior. One of the men, who said he had lived on that corner much of his life, said he even tried to follow the criminal scrapper and his accomplice once. His calls went unanswered by the school district, he said, and the scrappers did their destruction mostly at night.” The tragedy was compounded, according to one of the neighbors, because the school had been recently fitted with high-speed internet connections to promote a science and technology curriculum.
When I jumped into the old school, I saw newly built science labs completely trashed, eerily similar to how ISIS extremists would destroy monuments of culture and civilization in Iraq and Syria. But in Detroit’s case, the vandals were not crazed religious radicals, they were local residents, scavenging for scrap and destroying either for pleasure, anger, or both.
You can watch this June 2015 Detroit area news report on the scrapping at Crockett–all caught on live footage, with impunity. As one resident trying to protect abandoned public schools said, “How we can we hold off scrappers when we don’t have a license to arrest.”
Who really cares about Detroit’s decline or its public schools?
Today, the DPS is rated the worst in the nation for test scores. In May 2016 The Atlantic reported, “… the country has probably never witnessed an education crisis quite like Detroit’s.” And, then to no one’s surprise and certainly not to anyone in Detroit, no one really gave a crap. What happens in Detroit no longer seems to matter, no matter how awful and absurd.
After my trip to Detroit, I spent about four months trying to get respected Portland universities to host a lecture and photo show (click on the link to see how I presented the concept) on the decline of Detroit and how it looked in 2015. I was turned down by Portland State University, my alma mater Reed College, the University of Portland, and the Multnomah County Library. I made repeated requests to multiple faculty and these organizations.
The topic may just be too depressing or impossible to comprehend. Even worse, the story about mostly black Detroit and its current woes, like the simple destruction of one fine public school by the community itself, did not fit a narrative of race that is preferred many people at this time. A dominant narrative will always defeat an alternative story, particularly one that is rooted in ugly reality. I suspect this yawning disinterest was a combination of all of these factors.
To accept the reality of what Detroit is requires confronting the larger, painful issues about the United States that have not been addressed by our national political system. What we see instead are two candidates vying for the presidency who have used Detroit as a prop and photo-op to tell an economic story that does not resonate with the lives of people struggling in the city. Those two candidates, Donald Trump and Hillary Clinton, know little to nothing about the ordinary people in Detroit and have never stepped into any neighborhood where schools are abandoned, houses are burned, and blocks have gone feral. If one day one of them or any presidential candidate actually visit a place like Crockett, then I will retract this judgement
But let’s be honest. No one running for the nation’s highest office will ever see or want to see the real Detroit.
In researching material for my forthcoming book on the institution of American adoption, I have been collecting stories along with historical documentation and photos of the hospital where I was born in Detroit. [Author’s note, March 2019: my book is now available in paperback and ebook; you can also find an updated version of this article, with footnotes and a bibliography on my book website.]
The Florence Crittenton Home and Hospital in Detroit, taken in 1932. Source: Fifty Years’ Work with Girls, 1883-1933: A Story of the Florence Crittenton Homes.
At the time of my birth, the facility was called Crittenton General Hospital. It was created by the National Florence Crittenton Mission, a group started in 1883 to serve prostitutes, fallen and vulnerable women, and women who were pregnant out of marriage. This was a social group who were exploited and scorned, and the organization sought to assist them by giving them shelter, training in remedial women’s occupations, and, if possible, the space to build new lives.
As the mission’s 1933 publication states, the organization sought to rescue “young girls, both sinned against and sinning,” and to restore “them to the world strengthened against temptation and fitted in some measure to maintain themselves by work.”
In 1933, a half century after its founding, the organization had already served half a million women. Nearly all were white, and they were cared for around the country and even Canada–from sunny Florida, to rainy Oregon, to my home state of Michigan.
The Crittenton mission was uniquely reformist in the American progressive tradition. It was also deeply faith-based. Its strong public-health orientation proved equally important. It tried to improve the health and livelihoods of vulnerable groups and took an active role in training the newly created class of professional social workers.
Source: Fifty Years’ Work with Girls, 1883-1933: A Story of the Florence Crittenton Homes.
This combination made it a distinctly American institution. It touched the lives of generations of women who passed through its doors, and equally the children who were born either at the Crittenton homes and hospitals or cared for before and after the mothers’ pregnancies.
I am one of those persons who benefited from the organization’s original charitable mission. I was born in one of its hospitals.
But the organization’s much later and more hidden role in promoting adoption as a “solution” to out-of-wedlock pregnancies by the early 1960s had a much larger role. The solution in my case led to my relinquishment into foster care and eventual adoption. The hospital’s transformation during the boom years of American adoption occurred in the years surrounding my birth. Shortly after, in 1971, the hospital severed its ties with the national organization, ending an important chapter for an institution that played a critical role in Detroit’s social and medical history.
Preaching the gospel and saving lives
The mission began in New York City, under the guidance of businessman Charles Crittenton. A deeply evangelical man, he committed to helping one of society’s most vulnerable groups after the death of his 4-year-old daughter Florence from scarlet fever. Her demise created a deep bout of anguish. His autobiography describes how he turned to solitary prayer and saw the light, leading to his future mission. Today that mission lives on in the National Crittenton Foundation, now located in Portland, Oregon, my current home town. It is now dedicated to serving young women who are victims of violence and childhood adversity.
Charles Crittenton, founder of the National Florence Crittenton Mission.
At its start, in 1883, Crittenton worked the streets and promoted the Christian gospel, specifically to combat prostitution and provide service to exploited women and girls. The organization’s 50-year summary notes, “In its beginning the objective of Florence Crittenton efforts was the redemption of the fallen woman, the street-walker, and the inmate of houses of prostitution. The great agency in such redemption was the simple one of religious conversion.”
The organization slowly expanded its efforts, finding champions in many U.S. cities: St. Petersburg, Detroit, Boston, Nashville, San Francisco, Phoenix, Portland, and more. By 1895 he was joined by activist Dr. Kate Waller Barrett, with whom Crittenton corresponded. She later became the only woman on the national Crittenton board, after it was incorporated by Congress in 1898.
The mission was involved in anti-prostitution efforts during the early 1900s and focussed on training that would enable women to leave prostitution. Its primary focus remained on the rescue and care of unwed mothers, providing them appropriate medical care, and their right to raise their children free from the scorn of society.
Kate Waller Barrett, former president of the National Florence Crittenton Mission.
By the 1920s, Crittenton policy opposed separating a mother and child for adoption and believed that children should be kept with their birth mothers. As the mission’s 50-year history notes that promoting this policy helped to deepen the “love of the mother for her child and strengthening her desire to keep her baby.”
Motherhood was viewed as a means of reform. A Crittenton home became the place to promote both responsible motherhood and self-support. “Our girls need the influence of child-life upon them. They need to have the qualities that are essential to a strong, well-regulated character trained in them,” wrote Barrett in an undated pamphlet that described the mission’s philosophy of keeping mother and child together.
Crittenton combats the stigma of illegitimacy and helps “fallen women”
Nationally, the mission also sought to combat societal stigma for children associated with illegitimacy. By the second decade of the 20th century, publicized exposes had revealed the horrors of illegitimately born babies–the bastard children scorned by family, church, and most of society in the United States.
One highly publicized 1914 report called the Traffic in Babies by Dr. George Walker reported virtual charnel houses for unwanted, abandoned, and illegitimate children. These reportedly operated to “save” the single women from the disgrace of being unmarried mothers. The mortality rate of the relinquished bastard children was as high as 80 percent. Some doctors, nurses, midwives, clergymen, and hospital administrators actively referred the disgraced mothers who had sex out of marriage and became pregnant to these lethal, for-profit baby shops. Some hospitals even made money secretively moving the unwanted children from hospital wards to the unsanitary baby homes where most died.
Thc Crittenton mission clearly understood that the stigma of illegitimacy for out-of-wedlock babies was the driving force that demonized both mother and child. Prophetically, the mission in 1933 foretold of larger changes a half century later. The mission’s 50-year history notes: “Nothing short of a revolutionary charge in the mores of the American people will put the unmarried mother on a par, socially, with the married mother. Until such change shall be effected and there is no longer any such person as an illegitimate child, the mother without a marriage ring will continue to be looked at askance by a large proportion of the population and will suffer, even occasionally to the point of suicide, the shadow of social and family disgrace.” By the 1990s, single parenthood largely was de-stigmatized, with one in every three children in the United States being born outside of marriage.
Barrett headed the mission after Crittenton’s death in 1909. She passed away in 1925. By the 1930s, when these photographs were all taken, the organization was providing charitable service to assist those “fallen women,” in order “to restore to her, as far as possible, this most precious asset of a respected standing in society.” At this time, this still meant keeping the mother and child together.
Crittenton Home, San Francisco
Crittenton Home, E. Henry Wemme White Shiled Home, Portland
Crittenton Home, Sioux City
Crittenton Home, Nashville
Crittenton Home, Pittsburgh
Crittenton Home, St. Petersburg
(Click on each photograph to see a larger picture on a separate picture page.)
These pictures of the Florence Crittenton homes, published by the mission, reveal they projected a public image of being well-to-do. The facilities were all found in respectable areas, but had their actual mission hidden by the facade of upper-class and upper-middle-class gentility.
Well-to-do business people contributed to these charitable facilities in the cities where they operated, including my current home town of Portland. Detroit’s efforts at fund-raising, thanks to the Motor City’s new-found wealth from its booming automotive manufacturing sector, led to $700,000 to support the construction of a new hospital–a feat no others could match.
Crittenton General Hospital, the largest in the United States
The first Crittenton home in Detroit opened in 1897 over a store on what is now Broadway Avenue. The operation expanded and moved to a Victorian mansion on Brush Street, also in downtown Detroit. Within six years, it had outgrown its capacity. At any given time, the home was caring for 33 women, not counting the children, according to the mission’s published records. Thanks to the successful fund-raising efforts by the city’s wealthy to support women’s organizations, $700,000 in donations helped to secure land and build a new facility. This was meant to replace the old home, which was reportedly then in a “colored section” of the city. In 1907, the mission opened the Florence Crittenton Hospital on East Elizabeth Street. It offered inpatient and private patient care for indigent and unwed mothers. By 1922, it was offering up to 30 beds for mothers and their children.
National Florence Critttenton Mission convention, 1932, Detroit.
The hospital and home on Brush street had already become established as a facility that trained new or resident obstetrician. It was certified by the board of health governing local clinics and affiliated with the Detroit College of Medicine and Surgery. By 1927, the hospital had outgrown its capacity to meet the need to serve vulnerable women.
The new Florence Crittenton Home and Hospital, as it was identified in the mission’s records, was opened in 1929 at 1554 Tuxedo Avenue, about three miles from downtown Detroit. The new facility had three wings. Two of the facility’s wings were devoted to the care of the single and pregnant women and their infants. The mission’s records from 1932 note these two wings had 115 dormitory beds, 100 cribs, 40 bassinets, and a nursery that served this ever revolving population. Special recreation rooms were devoted to caring for the infants, and the roof was used for playtime and exposing the babies to sun and air.
According to the mission’s records, the hospital supplemented its operational costs with a third wing. It offered medical care mostly to lower-income women and children and was certified by American College of Surgeons. However, the third wing was separate from the two wings for the unwed women. The public wing also focussed on maternal care and general surgery.
By 1950, the hospital had to expand yet again to meet the growing demand for services. A separate maternity home called the Florence Crittenton Maternity Home, located at 11850 Woodrow Wilson, was built and opened in 1954. It was less than half a block from the hospital, which was then calling itself Crittenton General Hospital. The hospital and maternity home were connected by a service tunnel. The home could accommodate up to 60 young women, who had semi-private rooms. The home offered them class instruction, an auditorium, a dining facility, and even a “beauty shop,” according the mission’s records.
“Every effort was made to maintain a homelike atmosphere for the patient,” according to the official records. In reality, the young women were cut off from family and friends and faced with one of the most momentous decisions of their lives. In many cases, they would be pressured by a social workers, maternity staff, and medical professionals to relinquish their infant children to adoption.
Crittenton General Hospital was the largest of all Crittenton facilities in the country in the 1950s. Crittenton maternity homes–and in the case of cities like Boston and Detroit, combined Crittenton homes and hospitals–had become way stations. Pregnant women from their teens to their early to mid-20s stayed out the last days, weeks, or months of their pregnancy.
Meanwhile the hospital was reorganized after the home had opened. Only one floor of one wing was reserved for “unwed mothers,” like my birth mother. These single women mostly stayed at the maternity home next door. I was born in that wing dedicated to single women, most of whom would never see their children again. There was also a nursery to care for babies. The rest of the hospital’s 194 beds provided private hospital care, including obstetrics, surgery, and pediatric services.
The hospital also continued to be a training facility for residents, from the University of Michigan and Harper Hospital. In my case, the obstetrician who delivered me was completing a residency. He came from overseas, like many other doctors who arrived in the United States and were employed to serve low-income and high-needs patients in inner-urban and rural hospitals. When I contacted him for an interview, he told me how the hospital provided basic maternal services but also doubled as a residence to single and pregnant women, who lived next door at the home. He remembered the many “girls,” as he called those young, pregnant boarders. He suggested they worked in the facility, likely to pay part of their expenses.
In many cases by the 1960s, those women who stayed at Crittenton homes and hospitals were relinquishing their children to adoption agencies, at the urging of social workers, family, faith-based groups, churches, and the systems that were created to address out-of-wedlock marriage and illegitimate children. This marked a radical change from the original Crittenton mission to keep mothers and children together. This coincided with societal change that led to hundreds of thousands of unplanned pregnancies and the American social engineering experiment that promoted adoption as “the best solution” to both restore fallen women and find homes for the estimated 2.4 million illegitimately born babies placed for adoption from 1951 through 1973, the year of the landmark Roe v. Wade decision legalizing abortion in the United States.
One Crittenton center, in Sioux City, Iowa, claims that 98 percent of Crittenton babies were given up for adoption after World War II. (To learn more about how maternity homes functioned in the era of adoption shame and secrecy from the 1950s through 1973, read Anne Fessler’s The Girls Who Went Away.)
A shot of some of the tens of thousands of babies relinquished for adoption through the maternity care facilities run by the National Florence Crittenton Mission. (Source: Sioux City Journal, “Wife of Nobel winner started life at Crittenton Center,” Sept.18, 2011.
Crittenton’s legacy serving single, pregnant women disappears from history
A couple of years after I was born, the Crittenton hospital had moved from its inner-city Detroit environs to suburban Detroit, in Rochester. It became known as Crittenton Hospital Rochester. This came immediately after deadly race riots in 1967 that shook the city and left 43 dead and burned more than 1,000 buildings. Detroit was beginning a five-decade-long decay as a once great American city to one that has seen its population fall from 1.8 million souls in 1950 to less than 700,000 as of 2015.
The city’s declining population and expenditures made the Crittenton General Hospital in Detroit too expensive to operate. Occupancy dropped in half by 1973. The Detroit hospital permanently shuttered its doors on March 22, 1974. At the time, I was still a young boy in the St. Louis area. I was completely oblivious to my true origins as a Detroit adoptee who was born and then surrendered into the status of foster child at one of the nation’s preeminent maternal care facilities that promoted adoption. Only decades later I finally pieced together my life and discovered that I literally arrived into the world at the center of the American Adoption experience and experiment.
In 1975, the facility that served as the starting place in life for a generation of adoptees was demolished. The home remained open, run by the Henry Ford Hospital. Though Crittenton General Hospital was reduced to rubble and built over, its ghosts linger in the memory of thousands who were born there or who gave birth there. The former locations today of the hospital and home look more like a war zone, due to Detroit’s struggles to address economic decline and blight.
The suburban hospital that fled from the Motor City is now called Crittenton Hospital Medical Center. The facility’s current web site shows no record how the former and original Detroit facility once served a critical societal and local need helping vulnerable women and children.
Throughout August 2016, I have reached out with multiple emails and phone calls to the hospital in and its communications staff. I have not received any answer to many questions I submitted concerning the hospital’s older records about its service to those woman and adoptees like myself. I did receive some copies of official of pages from an official National Florence Crittention Mission commemorative book, but no answers concerning the number of births and adoptions that were performed at the hospital. I was told in one curt email reply, “Unfortunately we have no historian on staff, however, the website does have a brief description of our history. … Good luck with your endeavor.” Those birth and adoption records may not be available, or the hospital may be intentionally choosing not to draw attention to its former mission serving single, pregnant women and their bastard babies, like me.
The hospital in 2015 reportedly was bought by the St. Louis-based Ascension Health, a Catholic-run care system. It seems far from coincidental that a Catholic-run medical system would downplay or even omit critical historical information how one of its facilities had dedicated decades of service to those who got pregnant out of marriage and paid the terrible price that many organizations, including America’s many Christian faiths and institutions, exacted on those woman and their children. As an adoptee, I find this deeply saddening and at the same time no surprise at all.
It appears the shame and stigma of illegitimacy that the original founders of the mission sought so hard to overcome have not gone away at all in 2016. I doubt any of the tens of thousands of Crittenton babies like myself are surprised.
This article was first published on Sept. 3, 2016. It was last updated on Sept. 13, 2016, after I found additional original source material outlining the history of the Crittenton mission in Detroit. I have found two different names for the hospital of my birth: Crittenton General Hospital and Detroit Crittenton Hospital. Because of this inconsistency in officials records, I have updated this blog and will use the former, which is cited more frequently.
“But despite what you may think, good luck is more dangerous than bad luck. Bad luck teaches valuable lessons in patience, timing, and the need to be prepared for the worst; good luck deludes you into the opposite lesson, making you think your brilliance will carry you through. Your fortune will inevitably turn, and when it does you will be completely unprepared.” … Robert Greene, The 48 Laws of Power
During a recent outing to one of Seattle’s many brewpubs, I swapped stories with my good friend about hospital visits. Most people I know have had them, and a rarefied few have not. In my case, I have been hospitalized at least a half-dozen times, mostly for stitches, but also worse.
I told my friend some of my greatest learning moments came with contemplation lying in a hospital bed. There is nothing like pain one feels in the ugliness of a hospital room to focus the mind and to allow one to make sense of all the things that preceded the unforgettable trigger moments.
South African born psychiatrist and author Norman E. Rosenthal
South African born psychiatrist Norman E. Rosenthal has written a book on this theme called the Gift of Adversity. Thinking back on his own Apartheid-era life, surviving a near fatal stabbing, and his professional experiences, Rosenthal argues that innovation, resilience, and understanding emerge from our own adverse experiences and by gaining wisdom from those hard times. Writ large, economists will even refer to collective behaviors among entire generations, such as young people who came into adulthood in the Depression era, and whose lifelong buying patterns and decisions to live more austerely can be quantitatively measured.
Using examples of individuals who endured suffering yet who came out stronger, Rosenthal sees opportunity in these struggles for all of us. “Well, when adversity comes, the last word that comes to mind is gift, because it just looks like an unmitigated disaster. But, how many times have you heard a friend or somebody say, ‘You know, at the time, it seemed terrible, but in retrospect, it was for the best.’ … The first step is really to accept that the adversity has happened. … We have to somehow come to terms that it really has happened. Then, we have to analyze the situation, every adversity is different, and respond accordingly.”
My own experiences mirrored these points, almost too perfectly. Both involved small misfortunes with lifelong rewards.
Lesson No. 1: When I was 14 and not fully mature, I did something that was likely one of the dumbest acts of my life. I will not say exactly what it was, but it substantially disrupted life at my often-violent and chaotic junior high school, in University City, Mo. I was soon on my way for an expulsion as the second-to-last-day of classes was ending in June 1979.
Coming back to campus I encountered four guys who I did not know. At least three were students. The other may have been a high school student. He was older, a guy with a cast. They were tough. I was not. They were experienced in the art of violence. I had few such fighting skills. They were skillful manipulators, and I fell for small talk that drew me close. It turns out one of them had been blamed for the incident. That is the story I heard second-hand, and the group was bent on physical vengeance.
I do not remember everything that happened, but I do remember feeling a floating feeling. I was cold-cocked in the face by one of the four wearing a cast. I was bleeding profusely from a cut on my eyelid and could not see out of my left eye. I was lying on the ground not sure what had happened. I felt warm blood on my hand.
I remember the four of them mocking me and telling me if I was happy now about having the heat fall on them. It was a perfect example of the violence I had witnessed many times before at this school, often with the tense black-white racial undertones, and I am sure that tension influenced this assault too. They walked away, never having been arrested, never having been questioned by anyone, ever.
Insult piled upon injury. I had to go back to school, get kicked out by a furious principal who did not express any concern about me having just been assaulted on school grounds, and then have teachers sign my expulsion papers. One thug laughed at me in the hall and yelled, “What happened to you.” I shot back, in my un-masculine voice, “What do you think happened.” He turned cold, came close, and threatened, “Yo, want another one, mother fucker.” Luckily I walked away from that one.
I stayed at this hospital for nearly a week after I was assaulted and nearly blinded in my left eye, which proved to be a great learning moment.
My mom, a new teacher that year in the same district, took me to the emergency room in Barnes Hospital in St. Louis, where I was put into a shared room and monitored. My eye pressure was dangerously high because vessels were ruptured from blunt trauma, and I was at high risk of blindness in my left eye. The doctors prescribed having both eyes covered for more than a week to keep them from moving, lying in a bed, and having no physical activity.
I remember the slow passage of time and mostly the sounds of the ward, the voice of my few visitors, and the stories of a young man next to me going into eye surgery, not sure what would happen.
The school principal came once, talked briefly, and somehow waived my punishment as a result of being a violent crime victim. He never told me or my mom what the school or school district had done to investigate the assault. My mom told me years later she was too afraid as a new teacher to make waves with her new employer. No police officer ever took my story. The whole thing was wiped under the rug.
Lying there, in a flimsy hospital gown, feeling like needles were piercing my eyeball, I came to the realization of how precious my sight really was, and how close I had flirted with genuine disaster.
Lesson Learned: This was the clearest teaching moment ever in my life. Never, ever, do stupid things. Such acts have unforeseen consequences, particularly things that put you in a weak position with uncaring bureaucracies and with men who use violence to settle a score. If you act badly and unwisely without thinking, the sword of blunt justice will be swift, and it will be lasting. Also, without any allies or friends, one can be quickly abandoned by any organization if you are perceived as lacking advocacy skills and are vulnerable. So, do not present yourself as weak or easily exploited. Finally, and most importantly, always know exactly who you are dealing with when you confront strangers in strange circumstances. Trust your instincts, and keep your wits about you, always. Your instincts will always know who is a friend and who is a foe. Worry about bruised feelings later, from a safe distance.
It took me a whole summer to recover, and I could not engage in full physical activities for three months. I wore an eye patch half the summer. Decades later, I still have damage to the back of my eye that my most recent visit to an optometrist confirmed. He could see the damaged areas after my pupil was dilated.
Lesson No. 2: In my last month of my journalism master’s program at the University of North Carolina at Chapel Hill in July 1993, I was playing pickup soccer at the UNC-CH campus. It was supposed to be friendly, but of course men are fiercely competitive. A guy who I was marking intentionally head-butted me with the back of his head into my face. He broke my nose instantly, and it began to bleed profusely. I walked myself to the UNC-CH hospital, as it was close by.
This is how I looked shortly after my nose was broken and then reset in July 1993.
I waited about three hours for a resident to attend to my situation. The plastic-surgeon-to-be had been up about 28 hours and was in a terrible mood. After shooting cocaine painkillers into my nasal cavity area, he stuck a metal rod up my nose and proceeded to move things back into place. I recall screaming like a wild animal so loudly that it clearly disrupted patients in the entire wing. The exhausted and overworked resident was furious with my uncooperativeness, as he called it. He stuck the rod back in and went back to work.
A nurse came in and saw the procedure. She simply held my hand. I stopped crying. I instantly calmed down. My level of pain subsided dramatically. The compassionate act of human touch proved more powerful than any medicine. After the resident stuffed both of my nasal passages with some sort of medical gauze, I thanked the nurse. She gave me a caring look that said, everything’s going to be OK.
That night I wrote a poem about the war in Bosnia, then raging at the time, and I put my small problem into a larger perspective of suffering felt more severely by others around the world.
Lesson Learned: Human compassion and human touch are among the most powerful healing agents in the world, often more powerful than medicine and actions of medical specialists. The mind, when it needs to, can calm down and can process a stressful situation. Set the calming effect in motion, and show mindfulness of yourself and others who may be less fortunate.
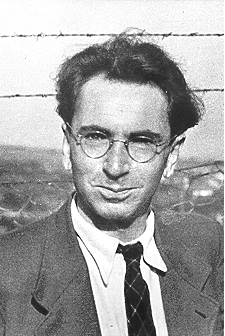
Comment: Author Rosenthal, who sees the importance of adversity, profiles the late Austrian neurologist and psychiatrist as well as a Holocaust survivor Viktor Frankl. He was the only member of his family to survive the genocide, staying in four different camps, and went on to receive acclaim for his widely read treatise called Man’s Search for Meaning, original published in German in 1946 Trotzdem Ja Zum Leben Sagen: Ein Psychologe erlebt das Konzentrationslager.
Holocaust survivor, psychiatrist, and author Viktor Frankl
Frankl’s own horrific experience taught fellow psychiatrist Rosenthal critical lessons also, that one can find meaning even in the midst of terrible adversity and that no single group of people is pure good or evil. Both types of people can be found in all groups, everywhere.
“It did not really matter what we expected from life, but rather what life expected from us,” wrote Frankl. “Our answer must consist, not in talk and meditation, but in right action and in right conduct. Life ultimately means taking the responsibility to find the right answer to its problems and to fulfill the tasks which it constantly sets for each individual.”
In no way did anything I experience come close to the challenges Frankl and other tough and lucky individuals have endured from such crimes.
I do know that in my case, my invaluable teachers came disguised as sterile wards and rooms of hospitals, giving me opportunities to contemplate larger truths. In one case, I created my own folly but could use my intellect to evaluate my mistakes. I also benefitted from being in hospitals, where I seldom felt kindness and felt great stress and also fear. This was clearly a place to avoid at all costs. I was doubly motivated to stay healthy—mind, body, and soul.
The wisdom I gained at those small junctures far exceeded anything I received in any university setting. As Robert Greene’s opening quote aptly notes, our bad luck prepares us for misfortune and gives us the strategies to overcome the roadblocks we build for ourselves or encounter from others. Those who are blessed mostly by good luck will eventually see their luck change, and when they do, they will be overtaken by those who have adapted and learned already.
So be thankful for those learning moments. They are your teachers, and you profit immensely by employing that knowledge wisely in the future.
Amazon, despite its critics, has been an innovator in the private sector.
The business press and the communications teams in the private sector work hard to show that innovation mingles in the air like oxygen at successful businesses. The theory goes, innovation breeds success, which creates profits, which spurs new products and services and wealth, which of course is good for the economy and thus all of us.
Forbes, for instance, showcases business innovators, like Starbucks and Amazon, by highlighting metrics that the magazine considers to be markers of innovation. According to the Forbes’ Sept. 2, 2013, piece on innovation, Amazon’s CEO Jeff Bezos says he looks for traits in innovators in his company and allows for innovation to occur three ways:
Rewarding innovators who are relentless in their on their vision but flexible on the details of how to get there.
Fostering a decentralized work culture for new products or services, so that the majority of employees feel like it is expected of them (Amazon’s now famous “two-pizza teams”).
Third, teaching teams how to experiment their way to innovations.
But once we start talking about government, talk of innovation gets tossed out the door. In fact, the prevailing wisdom among many in the private sector, and likely in the public sector too, is that government is the ultimate death machine to innovation.
Not only does innovation die still-borne in public agencies, government regulations themselves kill innovation in the private sector, many writers and politicians claim ad infinitum.
Do any public agencies have capacity to innovate?
Government still funds innovation and research and development, particularly in defense and health care. But as a culture, government is not the incubator, goes prevailing wisdom. One global survey completed this year puts trust in government around the world below 50%, behind trust in business at about 58%, for its ability to demonstrate change and new leadership.
Public health, as a public endeavor in the United States, is by definition a public undertaking. Thus it remains government-funded, government-run, and thus, be default, the inheritor of government’s best and worst traits.
As someone who has now worked at the international, state, and local levels of government, including in public health, I can attest to government bureaucracies’ failure in many instances to embrace change, inability to stimulate ideas, and poor track record in adopting new ideas to improve how government does business.
One recent research paper by British researchers Geoff Mulgan and David Albury on the lack of innovation in the public sector noted: “Most service managers and professionals spend the overwhelming proportion of their time dealing with the day-to-day pressures of delivering services, running their organisations [sic] and reporting to senior managers, political leaders, agencies and inspectorates [sic]. They have very little space to think about doing things differently or delivering services in ways which would alleviate the pressures and burdens.” In short, government culture lacks innovation.
The pair argue that innovation should be a core activity of the public sector. They claim this helps public services improve performance and public value, respond better to the public’s needs, boost efficiency, and cut costs.
Geoff Mulgan and David Albury ‘s diagram how public bodies do not innovate.
What are people saying about innovation in public health and health care
Developing more coherence between policies in the fields of education, research and innovation.
Measures to develop an innovation culture in universities.
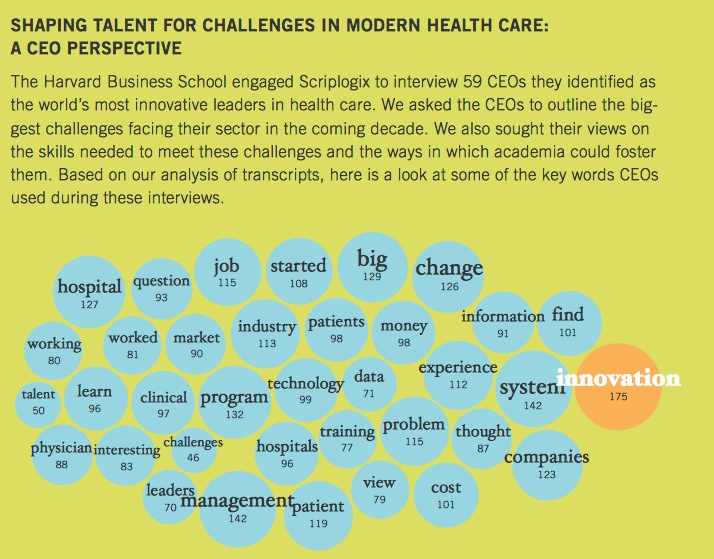
Back on this side of the pond, the Harvard Business School held a conference on innovation in the massive health care sector in October 2012, and then published a study in February 2013 on how innovation was seen as critical to health care and health education, which includes public health.
The report found that 59 of the CEOs of the world’s largest and most innovative health-sector organizations most frequently used the word “innovation.” According to the discussion of the attendees, innovation in its broadest sense was even seen as the “only way that change will happen and that creative solutions will be found for our current problems in health care.”
The most important characteristic for a company according to leading health care CEOs is innovation.
Recent evidence shows that innovation can lead to better outcomes. A 2013 study published in the Journal of Multidisciplinary Healthcare, on technological innovation and its effect on public health in the United States, found a correlation regionally in parts of the country where it was perceived that technological innovation was occurring. The study reported that “relationships between the technological innovation indicators and public health indicators were quantified,” and it was found “that technological innovation and public health share a fairly strong relationship.”
Will innovation remain a dirty word in public health departments at all levels of government?
But does anyone working in a local health jurisdiction, hard-strapped for cash in the post-Great Recession era of downsizing, see innovation taking place in their work environments? As hierarchical bodies, modeled originally after the military since their original inception in the United States, public health bodies are seldom discussed in organizational behavior literature as “innovative.” They are organized hierarchically and often divided by departments with no interchange, and their managers may be unable to allow for information sharing and promote collaboration seen in many for-profit firms.
Yes public health jurisdictions, to win much-coveted accreditation by the national Public Health Accreditation Board, must prove they are committed to quality improvement and a competent workforce. But this by no means is the same as encouraging a culture of innovation to adapt to tremendous change, particularly financial downturns and the challenges posed by chronic disease and the increasing wealth disparity among the top wage earners and the majority at the bottom, which is leading to great health disparities.
One local health jurisdiction that is trying to innovate, the Spokane Regional Health District, developed a strategic plan that calls out as its top two strategic priorities: increasing awareness about the role of public health and securing more stable funding. I think these are spot on and demonstrate how this agency has moved its focus upstream and is adapting itself to succeed in that bruising political arena.
But my own sense of public health jurisdictions, small and large in the Pacific Northwest at least, is that other jurisdictions may not wish to emulate Spokane because of agency rivalries and personal jealousies among upper management. I would love for one day to learn that some of the traits of private sector organizational behavior practices, such as rewarding innovators, promoting a culture of innovation, and teaching workers how to innovate take root. Right now, I’m not seeing that within the sector, and the talk is not matching the walk.
Thanks to everyone who has taken time to visit my blog focussing, mostly, on public health and health. I continue examining issues with the additional perspectives of history, culture, personal experience, and enterprise journalism. This month I crossed the 20,000-views threshold. See the screen snapshot below, taken today.
WordPress’s outstanding analytics tools provide a snapshot how many visitors and views have been recorded, in November 2013, and since I launched this blog in late March 2012.
WordPress’s analytics also report the following categories and tags attracted the most eyeballs:
Tags & Commentaries: Most popular topics you’ve written about
Topic & Views
Public Health 81
Health 77
Travel 57
Obesity, Sweden, Sweden, most beautiful women, Sweden has the world’s most beautiful women, infant mortality, life expectancy, Norway, Nordic Countries, public health systems, national public health investments, beauty stereotypes, national stereotypes, national obesity rankings, fat countries, obesity health threats 51
Photography 18
Native American 12
Africa 11
Human Rights 10
History 10
The most popular post on my blog looks at why Swedes have a reputation for being attractive, and whether that is related to the country’s strong public health system and universal health care. No doubt a fair number of visitors came looking for pictures of blonde Swedes in bikinis, but hopefully came away with some knowledge of how investing in health upstream can pay dividends that are linked to, yes, physical appearance and overall health.
The data are great validation for the idea that first launched this enterprise. It began during a spirited discussion at the University of Washington School of Public Health about the value and validity of training future public health leaders to specialize in publishing in peer-reviewed journals as opposed to open-source communications like WordPress-enabled blogs or social media or non-scientific publications. This is a topic that is being debated by many seeking to improve public health’s relevance for the year 2013 and beyond.
Having public relevancy in the face of funding cuts remains a critical issue in the field of public health, which has seen its workforce at the local level shrink by 44,000 jobs, or nearly a quarter of all workers, since the start of the Great Recession. Budgets in local health jurisdictions have been slashed to the bone according to a national survey of those organizations by the National Association of County & City Health Officials (NACCHO).
In fact, I would recommend to anyone contemplating a career in public health, outside of epidemiology or biostatistics, to consider advanced degrees in law, business, or applied health like nursing rather than this field, based on the national employment data. Or future public health leaders can learn through other means how to integrate new tools of communications to engage the public with research, to build support for funding health.
In fact, those who now manage the nation’s graduate public health programs need to use the tools of program evaluation, which they teach in the nation’s finest universities, and engage in a serious discussion if their education model is still working and achieving longer-term goals and ultimately leading to a better public health system and healthier country.
How many MPH graduates in 2013 found jobs within six months? Is that number acceptable? Why train a workforce for many jobs that may not be in high demand or nonexistent, with skills that are not reaching a wide audience, thus preventing the public from knowing what public health is and why it matters?
This will remain a fundamental issue at the heart of the crisis facing the field today and for years to come. Meanwhile, I think there will continue to be a bottoms-up response to how the profession adapts to change in the new era of diminished resources. I hope that this blog will continue to be involved in that larger discussion, and the numbers show that at least some online readers are hungry for information in easier-to-access ways.