Thanks to everyone who has taken time to visit my blog focussing, mostly, on public health and health. I continue examining issues with the additional perspectives of history, culture, personal experience, and enterprise journalism. This month I crossed the 20,000-views threshold. See the screen snapshot below, taken today.
WordPress’s outstanding analytics tools provide a snapshot how many visitors and views have been recorded, in November 2013, and since I launched this blog in late March 2012.
WordPress’s analytics also report the following categories and tags attracted the most eyeballs:
Tags & Commentaries: Most popular topics you’ve written about
Topic & Views
Public Health 81
Health 77
Travel 57
Obesity, Sweden, Sweden, most beautiful women, Sweden has the world’s most beautiful women, infant mortality, life expectancy, Norway, Nordic Countries, public health systems, national public health investments, beauty stereotypes, national stereotypes, national obesity rankings, fat countries, obesity health threats 51
Photography 18
Native American 12
Africa 11
Human Rights 10
History 10
The most popular post on my blog looks at why Swedes have a reputation for being attractive, and whether that is related to the country’s strong public health system and universal health care. No doubt a fair number of visitors came looking for pictures of blonde Swedes in bikinis, but hopefully came away with some knowledge of how investing in health upstream can pay dividends that are linked to, yes, physical appearance and overall health.
The data are great validation for the idea that first launched this enterprise. It began during a spirited discussion at the University of Washington School of Public Health about the value and validity of training future public health leaders to specialize in publishing in peer-reviewed journals as opposed to open-source communications like WordPress-enabled blogs or social media or non-scientific publications. This is a topic that is being debated by many seeking to improve public health’s relevance for the year 2013 and beyond.
Having public relevancy in the face of funding cuts remains a critical issue in the field of public health, which has seen its workforce at the local level shrink by 44,000 jobs, or nearly a quarter of all workers, since the start of the Great Recession. Budgets in local health jurisdictions have been slashed to the bone according to a national survey of those organizations by the National Association of County & City Health Officials (NACCHO).
In fact, I would recommend to anyone contemplating a career in public health, outside of epidemiology or biostatistics, to consider advanced degrees in law, business, or applied health like nursing rather than this field, based on the national employment data. Or future public health leaders can learn through other means how to integrate new tools of communications to engage the public with research, to build support for funding health.
In fact, those who now manage the nation’s graduate public health programs need to use the tools of program evaluation, which they teach in the nation’s finest universities, and engage in a serious discussion if their education model is still working and achieving longer-term goals and ultimately leading to a better public health system and healthier country.
How many MPH graduates in 2013 found jobs within six months? Is that number acceptable? Why train a workforce for many jobs that may not be in high demand or nonexistent, with skills that are not reaching a wide audience, thus preventing the public from knowing what public health is and why it matters?
This will remain a fundamental issue at the heart of the crisis facing the field today and for years to come. Meanwhile, I think there will continue to be a bottoms-up response to how the profession adapts to change in the new era of diminished resources. I hope that this blog will continue to be involved in that larger discussion, and the numbers show that at least some online readers are hungry for information in easier-to-access ways.
Dr. Roger Gollub and his beloved golden retriever, Sophie, at the famous Balto statue in downtown Anchorage.
Five years ago today, on a cold Alaska night, I was awoken by a strange phone call left on my answering machine saying something had happened to my Anchorage friend, Dr. Roger Gollub. Confused, I called the emergency room at the Maniilaq Health Center in Kotzebue, a remote bush city in the Northwest Arctic Borough, 26 miles north of the Arctic Circle on the Chukchi Sea. Roger had flown there a day earlier on assignment—I was with him the night before. I could not believe what I heard. The medical personnel told me, with great difficulty, that one of county’s finest pediatricians and public health caregivers had died from injuries sustained on a trail just outside of town that night.
Dr. Roger Gollub, a career pediatrician with the U.S. Public Health Service’s Indian Health Service, never returned home from his short visit to care for patients in this mostly Native community. He, along with a coworker, were mushing on a shared-use trail in subzero weather, under Alaska’s majestic starry skies, when they were run over by a snowmachine. The driver had a criminal background and was under the influence of drugs and booze. It was about a senseless a crime as I could have ever imagined, and more brutal because of the injuries Roger and his coworker sustained. (Note, Roger’s colleague survived, but only after heroic procedures and months of recovery, all costing more than any non-wealthy person can afford.)
After a bitter scream of disbelief upon hearing the news, I caught myself and thought, what would Roger do. I then spring into action for the next 24 turbulent hours, and the years beyond. In fact, my response to Roger’s tragic passing continues to this day. I would never have gone back to graduate school and earned my MPH in 2012 had I not been inspired by Roger’s amazing life’s work. He remains the finest man I have ever known.
Roger Gollub’s good friend and champion in so many uncountable ways, Gunnar Knapp, stands by the spot where Roger was taken on Nov. 19, 2008. Thanks, Gunnar, for sharing this with all of us who cared about Roger.
Roger had just retired from a distinguished career, which included an epidemiological residence with the U.S. Centers for Disease Control and path-breaking work with Native American and Alaskan Native communities (details here). He was still working under contract serving his many patients, and thinking about an active life ahead, including research, time with his wife and two daughters, projects with the Anchorage Amateur Radio Club, and travels he long delayed. Roger’s death forever changed my life, but also in a good way. From that time on I vowed to work even harder at showing the type of leadership that Roger demonstrated throughout his life.
Though he was only 5’6”, Roger towered above his peers as a professional, and particularly as an exemplary caregiver who understood his young Native American and Alaskan Native patients and their families. He was named physician of the year by the national health agency he dedicated his life too. He had legions of fans across the U.S. Public Health Service who held him in the highest of regards.
At Roger Gollub’s “Celebration of Life,” hundreds of well-wishers offered condolences and happy memories of one of Alaska’s finest doctors ever (December 2008).
I saw hardened, even stoic and cantankerous men who knew him through his ham radio activities openly weep when trying to make sense of his death. (Roger was an advanced ham, who knew Morse code, and who brought amazing life into the local club.) I saw more than 500 mostly Alaskan Natives give him the highest honors normally bestowed only to revered elders. I heard dozens of stories describing how Roger helped and even saved their very sick children, all while preventing costly medical waste within a sometimes-inefficient bureaucratic health delivery system. That alone is amazing, and Roger never expressed cynicism about that system that often thwarted him and his seasoned colleagues.
This letter, published in the Anchorage Daily News shortly after his death, captured a sentiment that lit up the blog coverage of his passing, with comments pouring in nationwide: “I am sure I’m not the only one who feels a great loss with the recent passing of Dr. Roger Gollub. He was truly a man with a servant’s heart and had a tremendous impact on my family. As a pediatrician at the Alaska Native Medical Center, he has shown pure dedication to the Native community and loved each and every patient. He had a place in my heart and my children’s. Once, my daughter had to see another doctor while he was on vacation, and cried for her doctor to come back. The world will never see another with the same compassion, dedication, intellect, integrity and valor as he. I was privileged to know this man for six years and he will never be forgotten in my children’s heart and mine. Linda Tomaganuk Anchorage.”
On the darkest of days, Roger still managed to smile. He always took phone calls from worried parents–at home, in his car, on his walks, wherever. How many doctors take house calls, or personal calls, ever? That was Roger. That was the kind of leader he was. He breathed it. He lived it.
Roger demonstrated to me examples of the leadership that I admire most:
Emotional Intelligence: Roger demonstrated this trait that most researchers say is the best predictor of leadership. He never appeared flustered. His coworkers described his ability to bring chaotic situations under control, in hospital wards or during infectious disease outbreaks, with a calm, deliberative, thorough, and positive manner. It proved contagious, and he earned trust and credibility among his peers.
Understanding of and Respect from his Peers: Abraham Lincoln, America’s greatest politician, was infamous for his empathy and his ability to understand his friends and opponents, which helped him articulate decisions and policy choices that always seemed perfectly suited for the difficult challenges ahead. He knew where the audience was, and where he needed them to go. Roger was celebrated in the Indian Health Service for his true commitment to community based participatory research, for which he earned the deepest respect from his Native American medical professionals. Mention Roger to anyone who has worked in this community, and you will quickly learn of Roger’s deep and genuine appreciation for the community he served during his lifetime. I met a former career pediatrician in the Indian Health Service last spring and mentioned Roger’s name, and was greeted by the most contagious grin I had seen in months. One University of Washington School of Public Health faculty member, who specializes in the field of community based participatory research and who knew Roger in New Mexico, said unequivocally, “Roger was the real deal.”
Leading by Example: Dorris Kearns Goodwin’s portrayal of Lincoln’s wartime cabinet, his famous “team of rivals,” highlights Lincoln’s eventual winning over of Democrat Edward Stanton. Before the Civil War, the former Ohio attorney had ridiculed and mocked the then lesser-known Illinois lawyer as a “long-armed ape” during a legal case during which Stanton shunned Lincoln’s work. Lincoln did not hold a grudge, and he then sought out Stanton to run the War Department during the Civil War, because he had the right qualities to master a complex organization. Stanton later become Lincoln’s strongest ally. Lincoln’s ability to put aside personal grudges and genuinely collaborate even with his political rivals was not an act. It was genuine.
Roger treated everyone he interacted with, even those who did not return the courtesy, with respect. I never once heard him utter a bitter word or even cynical comments, even when I expected them. I have met few people who have demonstrated this trait. Roger had a work ethic paralleled by few. He put in 12-hour days and longer, never compromised his duties as a father or husband, and excelled at nearly anything he tried to do—medicine, engineering, ham radio communications, running, parenting, research, epidemiology, research. Roger adopted practices seeing patients that saved taxpayers tens of thousands of dollars, which his peers steadfastly noted at his funeral. He never sought glory, though during his life he was gaining a national reputation he could never even imagine.
The small guy in the front row, in the middle, is team captain Roger Gollub (University City Senior High School Track Team, 1973).
Roger particularly demonstrated this talent at University City High School, where he ran track and cross country. I attended the same high school, though ten years after Roger. Roger was the smallest man on an interracial track team, which was comprised of very large young men who towered over Roger. Racial tensions were real here, but so were the strong bonds. I know this school, and I can assure you this is a serious alpha dog environment and not for the faint of heart, particularly among young, competitive men. Roger’s peers voted him captain of the track team, because he pushed the bar farther and competed harder and ran faster than all of them. In short, he inspired them to do better. He never asked for that title. He earned it. He made his team a genuine competitor at the state level. Roger carried that excellence to Yale where he competed for the Yale track team as well. (Roger’s own running hero was Olympian Edwin Moses.)
Moral Vision and Visionary: Roger’s values were nurtured in his Jewish, middle-class upbringing in a diverse community, University City, Mo., which we both called home. (I lived next door to Roger, but only briefly overlapped when I was younger, as he was 10 years older.) It was an often-hard place to learn about racial differences, but also a great place to dream big about pursing a path that made a difference. Roger knew exactly who he was and what he wanted. He graduated class valedictorian in 1973, and never forgot his roots. His vision was, as his friends said, a mix of Mighty Mouse heroism mixed with the Star Trek prime directive to do no harm–and yes, these describe his actions and values as a doctor working cross-culturally.
At Roger Gollub’s celebration of life, his family assembled assorted “tools of the trade” he used to care for sick kids, and of course the famous lobster hat.
I never once saw Roger lose faith in others or in the inherent goodness of people. His service to patients, the core mission of the U.S. Public Health Service, and purposes far bigger than himself can be seen in every personal and professional choice he ever made. He demonstrated and articulated a clear, humane vision for health care, community, family, race relations, and society that he blazed intensely everyday, inspiring dozens if not hundreds by his example.
Don’t be fooled by that doctor you see in this picture with a goofy grin, and a lobster hat and Elmo toys. That was a master professional’s slight of hand to get nervous kids comfortable and the most conniving of change agent’s subversive and effective strategy to reform a health care system that has long forgotten how to put compassion ahead of egos and profits.
I have yet to meet anyone in the field of public health and public service who embodied all of the leadership traits Roger seemed to have in spades. Sometimes we just get dealt the right hand and can say, damn, I was lucky I had a chance to work with or know such a gifted, natural leader. Thanks, Roger!
The seal of the U.S. Department of Defense, representing seven branches of the U.S. military.
The U.S. Department of Defense (DoD) remains one of the most sophisticated media production machines on the planet. Its ubiquitous advertising filters into every aspect of our lives, from public schools to product placement in the lucrative gaming industry to traditional online ads.
In 2007 alone, according to a Rand Corp. study, the total recruiting budget for the Army, Navy, Air Force, and Marine Corps exceeded $3.2 billion. Rand Corp. analysts also deemed those investments as successful as measured by recruitment, even during two ongoing wars in Afghanistan and Iraq.
Events with military personnel always feature sophisticated press and social media coverage. One of the more nuanced and I think effective messages I have seen from the DoD is how the military is not just about defense, but about a more deeply and morally resonant “good.” The U.S. Navy’s very slick videos call the branch a “a global force for good,” and show Navy SEALs in action carrying that message.
This clip from a U.S. Navy recruiting video shows a successful branding effort by the U.S. Department of Defense to promote its global activities as a moral good, including special ops efforts by U.S. special forces.
Helping to prop up that messaging is the country’s long-standing integration of public health services into the DoD and overall military readiness. The military is successfully integrating public health activities, and it is branding these as part of its global efforts, including on the new battlefield in Africa.
Through contracting opportunities that support these efforts, many U.S. based firms who specialize in development and traditional public health activities are actively supporting these initiatives, in order to monetize their own business models.
Chasing contracts serving two masters: public health and defense
I recently stumbled on a job posted on the American Public Health Association (APHA) LinkedIn page by a company called the QED Group, LLC. The position was similar to ones I see posted on their job site now, for work on a “monitoring and evaluation” project in Africa.
This is one of many government-contracting agencies that chase hundreds of millions of contracts with U.S. government agencies and the major public health funders like the Bill and Melinda Gates Foundation.
In this case, the company was specifically targeting those in the public health community, who are entering the field or currently have positions with backgrounds in public health, economics, science, and health. The 15-year-old company itself actually began as a so-called 8(a) contractor, which means it could win no-bid and lucrative government contracts that are now the center of an ongoing and intense controversy over government waste. (These companies were created by the late Alaska Sen. Ted Stevens, who created the provision to steer billions in government contracting to Alaska Native owned firms that partner with companies like Halliburton and the Blackwater overseas and in the United States.)
The company QED Group showcases its recent work evaluating anti-terrorism-related efforts in North Africa.
Today, QED Group, LLC claims “it is full-service international consulting firm committed to solving complex global challenges through innovative solutions” by providing clients “with best-value services so they increase their efficiency, learning capacity, and accountability to the public in an ever more complex and interconnected world.” It lists standard international development and public health contract areas of health, economic growth, and democracy and governance.
QED Group is not the only multi-purpose public health and development agency chasing military and global health contracts in Africa. Another health contracting company called PPD boasts of its “long history of supporting the National Institutes of Health, the nation’s foremost medical research agency,” and that it was “awarded a large contract by the U.S. Army.” It claims its is also a “preferred provider to a consortium of 14 global health Product Development Partners (PDPs), funded in part by the Bill & Melinda Gates Foundation.”
As a public health professional, QED Group looks like a great company to join. However, if one scratches deeper, one learns that this company also uses its public health competencies with the U.S. military, which is spearheaded in Africa by U.S. Africa Command, or AFRICOM. This raises larger questions of the conflicting ethics of both promoting human health and public health and also serving the U.S. Department of Defense, whose primary mission is to “deter war and to protect the security of our country.”
AFRICOM’s emerging role flexing U.S. power in Africa
AFRICOM’s demonstration of “hard power” is well-documented through its use of lethal firepower in Africa. AFRICOM is reportedly building a drone base in Niger and is expanding an already busy airfield at a Horn of Africa base in the tiny coastal nation of Djibouti. On Oct. 29, 2013, a U.S. drone strike took out an explosives expert with the al-Qaida-linked al-Shabaab terrorist group in Somalia, which had led a deadly assault at a Kenyan shopping center earlier that month.
One blog critical of the United States’ foreign policy, Law in Action, reports that the AFRICOM is involved in the A to Z of Africa. “They’re involved in Algeria and Angola, Benin and Botswana, Burkina Faso and Burundi, Cameroon and the Cape Verde Islands. And that’s just the ABCs of the situation. Skip to the end of the alphabet and the story remains the same: Senegal and the Seychelles, Togo and Tunisia, Uganda and Zambia. From north to south, east to west, the Horn of Africa to the Sahel, the heart of the continent to the islands off its coasts, the U.S. military is at work.”
U.S. efforts in Africa require health, public health, and development experts. As it turns out the company, QED Group, won a USAID contract examining U.S. efforts promoting “counter-extremism” programs in the Sahel. That study evaluated work using AFRICOM-commissioned surveys, all designed to promote U.S. national security interests in the unstable area.
The area is deeply divided between Christians and Moslems. It is also home to one of the largest al-Qaida based insurgencies known as al-Qaida in the Islamic Maghreb, which has similar violent aspirations as the ultra-violent Boko Haram Islamic militant movement of violence-wracked northern Nigeria. Al-Qaida in the Islamic Maghreb military seized control of Northern Mali in 2012, which ended when U.S.-supported French military forces invaded the country and routed the Islamic extremists in January 2013.
Public health’s historic role with U.S. defense and national security
“Hard power” and “soft power” are tightly intertwined in U.S. overseas efforts, where health and public health personnel support U.S. interests. This is true in Afghanistan and is certainly true in North Africa. This particular QED-led program used the traditional public health method of a program evaluation of an antiterrorism program to see if a USAID program was changing views in Mali, Niger and Chad—all extremely poor countries that are at the heart of a larger struggle between Islamists and the West.
That research methods used in public health–and which I have used to focus on health equity issues in Seattle–can be used equally well by U.S. development agencies to advance a national security agenda is not itself surprising.
However, faculty certainly did not make that case where I studied public health (the University of Washington School of Public Health). I think courses should be offered on public health’s role in national defense and international security activities, because it is nearly inevitable public health work will overlap with some form of security interests for many public health professionals, whether they want to accept this or not.
U.S. Public Health Service Commissioned Corps members proudly serve their country and wear its uniforms. This photo published on the corps’ web site demonstrates that pride.
Public health in the United States began as a part of the U.S. armed services, as far back as the late 1700s. It was formalized with the military title of U.S. Surgeon General in 1870. To this day those who enter the U.S. Public Health Service Commissioned Corps wear military uniforms and hold military ranks.
A good friend of mine who spent two decades in the Indian Health Service, one of seven branches in the corps, retired a colonel, or “full bird.” He always experienced bemusement when much larger and far tougher service personnel had to salute him when he showed his ID as he entered Alaska’s Joint Base Elmendorf Fort Richardson looking often like a fashion-challenged bum in his minivan (he frequently had to see patients on base, and was doing his job well).
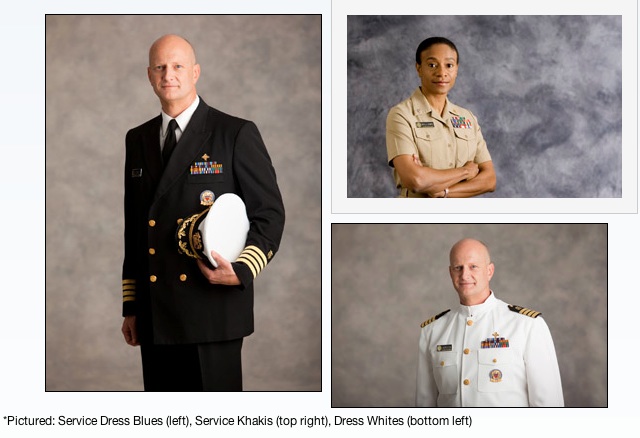
The U.S. Public Health Service Commission Corps’ web site shows the different uniforms worn by its members.
The U.S. Army’s Public Health Command was launched in WWII, and it remains active today. One of its largest centers is Madigan Army Medical Center at Joint Base Lewis McChord, in Pierce County, Washington. Public Health activities are central to the success of the U.S. Armed Services, who promote population-based measures and recommendations outlined by HealthyPeople 2020 to have a healthy fighting force.
AFRICOM charts likely path for the future integration of public health and defense
This screen snapshot of an AFRICOM media file highlights the public health and health related efforts AFRICOM personnel undertake in the region, where military efforts are also underway to suppress and disrupt Islamic extremist groups.
Today, the U.S. military continues to use the “soft power” of international public health to advance its geopolitical interests in North Africa. In April 2013, for example, AFRICOM hosted an international malaria partnership conference in Accra, Ghana, with malaria experts and senior medical personnel from eight West African nations to share best practices to address the major public health posed by malaria.
At last count, the disease took an estimated 660,000 lives annually, mostly among African children.
At the event, Navy Capt. (Dr.) David K. Weiss, command surgeon for AFRICOM, said: “We are excited about partnering with the eight African nations who are participating. We’ll share best practices about how to treat malaria, which adversely impacts all of our forces in West Africa. This is a great opportunity for all of us, and I truly believe that we are stronger together as partners.”
I have reported on this blog before how AFRICOM and the United States will increasingly use global health as a bridge to advance the U.S. agenda in Africa. And global health and public health professionals will remain front and center in those activities, outside of the far messier and controversial use of drone strikes.
It is likely this soft and hard power mission will continue for years to come. Subcontractors like QED Group will likely continue chasing contracts with USAID related to terror threats. Global health experts will meet in another African capital to discuss major diseases afflicting African nations at AFRICOM-hosted events. And drones will continue flying lethal missions over lawless areas like Somalia and the Sahel, launching missiles at suspected terrorist targets.
A long-abandoned Armenian church can be seen in the Karakoy neighborhood of Istanbul, Turkey, on one of the busiest streets of the largest city in the country.
In September and October 2001, I traveled throughout Turkey for more than three weeks. It was one of my greatest trips ever. I loved the country and really enjoyed my experiences getting to know the Turkish people. I recommend the country to anyone. During that trip, I worked on a photo-documentary project, visiting historic locations of the Armenians. I also visited many other places too, from ancient monasteries, to Greek and Roman ruins, to the wonders of the Ottoman Empire, to Kurdish regions that were experiencing disturbances that have not fully settled to this day.
I did a lot of research before this trip, and received a lot of assistance from some Armenian colleagues I befriended as a result of my interest in photographing remnants of the Anatolian Armenians, who experienced the first clearly documented case of genocide of the 20th century. I do not wish to get into a larger discussion of that topic. I am republishing a story, with photographs, that I published first in 2002. It recounts my travels to historic locations linked to the genocide and Armenian history in present-day Turkey.
I finally got around to publishing this story again, after finding some materials I had forgotten about–the story told through numbers. Since I work in public health these days, I find myself steeped in data and perhaps a bit beholden to it. So with that frame of view, I present a “by the numbers” perspective on my travels in Turkey, this significant crime against humanity, and a point of view that I try to keep in focus when I get lost in the small stuff and forgot the important stuff.
My story, An Armenian Journey, is in PDF format, and because of its large file size at 25 mb, it may take a while to download. Please be patient, as it well worth your time. A very useful map of the tragic events is published by the Armenian National Institute. A fine collection of historic prints and illustrations of now vanished Armenian communities in the Ottoman Empire in present-day Turkey can be found on the Houshamadyan web site. That site shows pictures of many of the places I visited, and you can compare historic pictures with the pictures I show in my story.
1.5 Approximate number of persons, in millions, estimated to have been murdered during the genocide against Armenian citizens of the Ottoman Empire during and after World War I.
.6 Approximate number of Armenians, in millions, that the Turkish government today claims died during World War I during what the government called a military uprising.
35 Number of Armenian churches still active in Istanbul, according to a custodian at the Kilisesi Vakfik in the Galatasaray neighborhood of Istanbul.
100,000 Approximate number of ethnic Armenians residing in Istanbul today, according to members of the Holy Mother-of-God Armenian Patriarchal Church, in the Kumkapi neighborhood of Istanbul.
30 Approximate distance, in meters, from the Kumkapi police station to the Armenian Patriarchate (main church for Armenian Christians in Turkey).
5 Number of recognizable historic Armenian religious structures in Erzerum that are either labeled Selcuk or unknown origin.
2,549 Number of Armenian ecclesiastical buildings in the Ottoman Empire (churches, monasteries, parish structures), according to a survey by the Armenian Patriarchate of Constantinople in 1914, on the eve of the genocide (source, William Dalrymple, From the Holy Mountain).
464 Number of Armenian ecclesiastical buildings in the Republic of Turkey that had disappeared from the total of only 913 structures with known whereabouts in 1974, according to a survey done of the buildings that year (source, William Dalrymple, From the Holy Mountain).
252 Number of Armenian ecclesiastical buildings of the 913 buildings with known whereabouts that were in ruins, according to a survey done in 1974 (source, William Dalrymple, From the Holy Mountain).
197 Armenian ecclesiastical buildings of the 913 buildings with known whereabouts that were in sound shape, according to a survey done in 1974 (source, William Dalrymple, From the Holy Mountain).
0 Number of references to “Armenia” or “Armenians” at Ani, the historic cultural capital of the Bagratid Armenian kingdom in eastern Anatolia on the border of modern-day Armenia and inside Turkey.
1/2 Number of surviving Armenian structures in present-day Kozan, called Sis by the Armenians, and the capital of their kingdom in Cilicia in the 13th and 14th centuries and formerly seat of the Armenia Catholicasate.
0 Number of references to Armenia on signs next to these structures.
350 Approximate number of mosques (including the great Suleymaniye and Selimiye mosques), bridges, and buildings credited to the Armenian architect Sinan.
1 Number of Armenian religious buildings remaining in Harput, the center of the graphic, first-hand account of the genocide by American diplomat Leslie Davis called The Slaughterhouse Province.
4 Number of monument structures at Liberty Hill in Istanbul to honor Talaat Pasha and the Young Turks, the principal architects of the first genocide of the 20th century.
0 Number of signs outside the now locked and gated memorial indicating the contents inside the weed-covered area originally built in 1943 to honor the former Turkish leader, who was gunned down in Berlin in 1921 by an exiled Armenian, Soghomon Tehlirian (in 2001).
2 Number of Armenian spires visible at Isak Pasa Palace, near Mt. Ararat, a complex that contemporary sources say was built by a Kurdish chief in 1685. [Structure is called a Turbet in Let’s Go.]
2 Number of military points passed prior to entering the Ani complex.
3 Number of government and police offices required to complete an Ani application process (taking a quick one hour of time, in 2001).
25 Approximate cost, in U.S. dollars (as of October 2001), to visit the historic Ani ruins.
0 Number of road crossings open to commerce and road travelers between Turkey and present-day Armenia (in 2001).
6 Number of Armenian churches I visited in Istanbul that are now permanently closed.
0 Number of references to “Armenia” or “Armenian” at Akdamar Church, an Armenian church outside Van on an island in Lake Van.
53 Number of days more than 4,000 Armenian villagers in the Hatay Province south of Antakya, on Musa Dagh (“Mountain of Moses”), resisted Ottoman forces in 1915 before they were rescued by Allied warships.
18 Number of languages that Franz Werfel’s best-selling account of the famous siege and rescue–Forty Days of Musa Dagh–has been translated into since its first publication in 1933.
24 The day every April that Armenians the world over mark as their genocide anniversary day, commemorating the date in 1915 that 600 leading Armenians and another 5,000 Armenians in Istanbul were rounded up, and almost all killed.
Recently I posted a link on my Facebook page to a Slate blog piece by Allison Benedikt: If you send your kid to private school, you are a bad person. It drew some negative feedback as well as a very positive response. Benedikt, who is a parent, provocatively suggests if you do this, you are “not bad like murderer bad—but bad like ruining-one-of-our-nation’s-most-essential-institutions-in-order-to-get-what’s-best-for-your-kid bad. So, pretty bad.”
Benedikt then goes on to argue that people who abandon public K-12 education undermine the foundations that make for a healthier, more democratic society. In defense of her seemingly provocative view, she claims that the bad things she did with bad kids during her public school days taught her more about life than reading Walt Whitman. In the end, she pleads with the middle-class moms and dads of the country reading her piece to go to bat for public schools in the most visceral way.
There’s a big public health story here too, but first, let me give some personal background and why this resonated profoundly with me.
How I endured then cherished my public school experience
I have friends who send/have sent their kids to private schools, and I do not think they are bad. But having attended K-12 public schools my formative years, I am very biased to Benedikt’s point of view. It’s my tribe, those public school grads. You might call me a bulldog on this point. My mother was a public school teacher as well, so I know the exhausting and harsh down sides from the perspective of such educators.
The most important things I learned about life are the ones I clawed together in that often chaotic petri dish, and at times it was chaos too. While I think many aspects of U.S. public schools truly stink, mainly the large mega schools and school systems that reward jocks and criminally fail to prevent abusive bullying of all stripes, I cannot deny the value of socializing in this publicly-funded mosh pit provides.
A snapshot from my graduating class of 1983 from University City Senior High School; yes I’m in there, bad hair and all.
The system I attended til 1983 in University City, next to St. Louis, was good (in some ways), but very divided in terms of who was on the fast track to say a great music college and who was on the fast track to say joining the armed forces. Both paths seem good to me now, and I was among those without a clear path. People came from respectable professional families (the ones whose parents were high-earning types like doctors) and from those living on the margins. The realities of race, and in my mind class, were omnipresent. During my years in that system, grades 3-12, the student population was roughly 70% black, 25% white, and 5% all other (Latino, Asian, Middle Eastern).
There were great teachers, and awful ones. There were clicks, stoners, nerds, punks, jocks, super achievers, motorheads (people I respected the most), future criminals, future drop-outs, future business people, musicians, and hip hop artists. Violence lurked in many places, too. I saw three extremely violent and criminal assaults (two on campus, one off) during a several-year stint. I experienced more than my fair share of racial harassment, and I was hospitalized after being cold cocked on a school setting—a crime I partially brought on myself, but also with racial undertones. But hey, who says high school is supposed to be walk through the flowers?
A group shot from my 1983 graduating class; I am not seen in this one.
In the end, I would not trade this for anything. All of this gave me the tools to deal with an increasingly diverse country, where skills at communicating cross-culturally matter in every professional setting, and in most personal interactions too. In a more fundamental way, I felt equipped to stand my ground and hold my own anywhere in the world, and really appreciate people on their own terms. It gave me a window to really get to know people.
Schools becoming less diverse and more segregated
Today, however, it is more likely students finishing their K-12 education will not have experienced something like what I did—a school that has true racial and cultural diversity without deep segregation at the district level. According to a 2009 report by the University of California at Los Angeles’ Civil Rights Project, schools in the United States are more segregated today than they have been in more than 40 years. Worse, millions of non-white students are trapped in so-called “dropout factory” (public) high schools, where large numbers do not graduate and remain unprepared for the challenges of an increasingly knowledge-based economy of technological haves and have-nots.
While our nation has come a long way since the Brown v. Board of Education Supreme Court case of 1954 made it illegal to segregate schools based on race, there are still many problems. A typical example is in Richmond, Va., where a recent news report found that 40 years after the U.S. Supreme Court rejected consolidation of public school districts to achieve racial integration in the Richmond area, one in every three black students in the Richmond-Petersburg region attends a school with a population that is at least 90 percent black and 75 percent poor.
So what right-minded parent, black or white or brown, would want their child in a school that is segregated and all but likely underfunded? It is a non-starter, really.
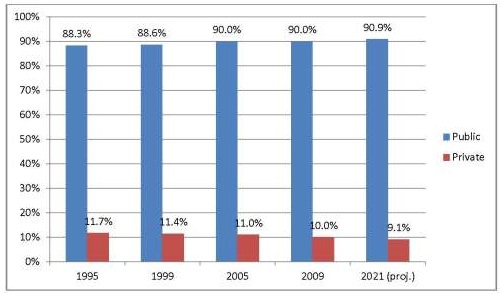
The U.S. Department of Education’s data show private school enrollment has dropped, mostly due to declining attendance at Catholic schools.
Public vs. private schools by the numbers
According to the U.S. Department of Education in 2008, the number of public schools in the United States outnumbered private schools (including religious schools) by about a 5-1 margin (65,990 vs. 13,864). In the past 15 years (1995-2009), private school enrollment actually dropped from 12% of all enrollment to less than 10%. The main reason is attributed to the drop in Catholic school enrollment.
Economic downturns also led to falling enrollment. Due to the increasing decline of the U.S. middle class and the concentration of all wealth in the hands of a few Americans, the disparities have even worsened. Between 2009 and 2011, the mean net worth of the wealthiest 7% of households rose 28%, while the mean net worth of households in the lower 93% slipped 4%, according to a Pew Research Center.
According to Jack Jennings, founder and former president of the Center on Education Policy, the real issue remains how well the nation will educate the 90% majority—the ones with increasingly less wealth—who are not privileged and have less resources and who comprise the majority of our public school student population. They will be the future soldiers, medical professionals, politicians, scientists, engineers, construction workers, and more. “If we want a bright future, we must focus national attention on making public schools as good as they can be,” Jenning says.
At last count, about 49 million kids were enrolled in K-12 education, or nearly or a sixth of the U.S. population. So the debate about where we educate these youngest citizens and our up-and-coming leaders is about as important issue as any we face as a nation, and as citizens of our communities and country.
Jessica Strauss, in a June 2013 New York Times piece on the country’s growing education divide, pointedly notes: “The truth is that there are two very different education stories in America. The children of the wealthiest 10% or so do receive some of the best education in the world, and the quality keeps getting better. For most everyone else, this is not the case. America’s average standing in global education rankings has tumbled not because everyone is falling, but because of the country’s deep, still-widening achievement gap between socioeconomic groups.”
Education, health, and ethnic diversity–fused at the hip
So where should kids get the tools they need to prepare them for their life challenges, a turbulent economy that is divided by knowledge and technology, and the diversity in a country that will be less than 50% white by 2043. Navigating the nation’s ethnic and linguistic diversity will be as critical for someone running a small business as it will be for a highly trained medical professional serving patients with different ways of dealing with health care.
Research over the past 20 years has generated countless studies consistently showing how a person’s health is driven largely by underlying factors, or the social determinants of health. In short, one’s education will predict a child’s future health as good as any other causal factor.
So as a nation, if we also want to promote opportunities for everyone to achieve good health, as well as good jobs, there must be a public policy imperative to ensure that the poor, underachieving, increasingly non-white public schools do not get short-changed. Does that mean more blog posts and rants chastising liberal middle-class parents and taunting them? Perhaps that’s one way to raise awareness, as Benedikt tried and I think succeeded.
But I’m less convinced parents of any race who want their kids to be learning Mandarin by age 8 and making high-def feature movies by grade 10 (like students do at the elite Annie Wright School of Tacoma, Wash.) will dare risk their child’s well-being for the larger social good. If parents are fortunate to be economically well off in that narrowing minority of “haves,” they will choose the high-price, high-quality schools like this leafy campus and pay tens of thousands of dollars for that rare privilege. Because I am not a parent, I can avoid this very hard decision, so I am very lucky.
Such advantage-bestowed kids will undoubtedly go on to be successful leaders. But I am less inclined to believe they will be the right leaders, who have a visceral sense of what’s best for all of us, though many of them will be the ones driving the agenda in many of the organizations that impact us the most.
Smallpox remains the only human disease that has been successfully eradicated. Its scourge has been global, impacting nearly every great civilization from the time of the Pharaohs onward.
In Europe, it reportedly claimed 60 million lives in the 1700s. In the 1500s, up to 3 million Aztecs died after being infected by the conquering Spanish, bringing about the collapse of their culture and civilization more effectively than the violent conquistadores could have ever dreamed. The last reported case occurred in the 1970s. Since that time, the virus has existed only in two highly guarded labs.
Smallpox is also tragically rooted in the meeting of European and Native American cultures, and its horrific impact on the continent’s first peoples underlies the nation’s historic narrative as much as political and economic developments from colonial expansion to industrialization to slavery.
The pilgrims, like the Spanish, brought the dreaded scourge, which immediately took a toll on Native tribes on the Eastern seaboard. The first outbreak claimed 20 of the white settlers’ lives. Founding Father Ben Franklin lost a son to smallpox in 1736. But smallpox more than any army, particularly in the Pacific Northwest in the Oregon territory, made it possible for the young American nation to conquer Native areas, many totally wiped clean of their Native inhabitants. I will talk more about the impacts in Oregon shortly, but first some background on the killer virus.
Smallpox’s enormous role in North American and Native American history
There are two smallpox variants, Variola major, the more severe form, and the less severe Variola minor. Its symptoms include fever and lethargy about two weeks after exposure, followed by a sore throat and vomiting. For those afflicted, a rash would then appear on the face and body, and sores in the mouth, throat, and nose. Infectious pustules would emerge and expand. By the third week, scabs formed and separated from the skin. The virus is spread by respiratory droplets, and also by contaminated bedding and clothes. This was how many historians suspect the disease may have been transmitted to Native Americans in North America.
French Jesuits in Canada in 1625, according to an account by Ian and Jennifer Glynn in The Life and Death of Smallpox, received great hostility from Natives because of the link made between the disease and contact with Europeans. The missionaries reported the local people “observed with some sort of reason that since our arrival in these lands those who had been the nearest to us had happened to be the most ruined by [smallpox], and that whole village of those who had receive us now appeared utterly exterminated.”
The first recorded use of smallpox as a weapon was during the siege of Fort Pitt in 1763, when Native tribes during Pontiac’s uprising during the French and Indian war were reportedly given infected blankets by a British general, possibly with the goal of infection, even though scientific knowledge at the time did not fully understand germ theory or microbial infections. However, there was an understanding of how the disease might be spread based on experiences. Reports also exist of the British attempting to infect colonial areas during the Revolutionary War–all early cases of germ warfare.
Smallpox was reportedly used against the 10,000-man contingent of the Continental Army that invaded British-held Quebec. Of that force, half were stricken by smallpox, and it was theorized the British commander may have intentionally spread it by sending infected persons to Continental Army camps. That army’s commander died, and the force retreated in 1776, keeping the Canadian territories intact and thus giving birth to Canada. Noted John Adams, “Our misfortunes in Canada are enough to melt the heart of stone. The smallpox is 10 times more terrible than the British, Canadians and Indians together.”
Abraham Lincoln supposedly contracted it during the height of the Civil Ware in 1863—the outcome of which could have turned the course of U.S. and global history, had he died. (I for one am glad he survived this.)
The first vaccine, developed in 1770, was derived from cowpox by Edward Jenner. He had observed how a milk maid was inoculated from the impacts of the more deadline Variola major and minor by a previous exposure to cowpox. It was not until 1947 when a frozen vaccine was introduced globally. After a costly global campaign, smallpox was declared eradicated in 1980.
The College of Physicians of Philadelphia has published an extremely useful illustration and timeline of the history of smallpox in the United states and globally.
It was less than 100 years ago smallpox wreaked havoc. A photo provided by Dr. Bennet Lorbar shows a man with pox marks on his body, among the victims of the 1925 Milwaukee outbreak that claimed 87 lives.
Today, many people in the United States, particularly those born after routine smallpox vaccinations were ended in 1972, have no memory of how awful such a disease can be. (The CDC has a plan to vaccinate the entire country should the virus ever break free from its labs.)
This may be a contributing factor to the rise of the anti-vaccination movement. It should noted opposition to smallpox vaccination in the United States dates to the 1920s, and opposition even as far back as the first vaccine of Jenners.
Ex-Playmate McCarthy and the vaccination deniers
The most famous case of modern day vaccination denialism is linked to controversies surrounding the measles, mumps, and rubella (MMR) vaccine, and its alleged link to autism and autism spectrum disorder. This bogus claim was completely based on a widely discredited study published by the British medical journal the Lancet in 2004, and then formally retracted in 2010. It was further debunked by extensive population based studies.
Facts, of course, have still not stopped former 1994 Playmate of the year Jenny McCarthy, and the “Green our Vaccines” campaign, from claiming toxins in vaccines cause autism.
Would anyone care what Jenny McCarthy has ever said if she did not have large breasts and was not the Playmate of the Year in 1994?
Her campaign of disinformation just got a boost when she was given a national stage by Walt Disney Co.-owned ABC News, which hired the vaccination extremist to its show called The View in mid-July 2013. She begins her post in September.
As expected a chorus of worried public health advocates and policy wonks decried ABC’s crass capitalistic gesture. This made no impact whatsoever on the parent corporation, Disney—all of which might lead a rational person to ask when the Disney-owned ABC News might hire a blond, big-boobed Holocaust denier to co-host a lively, unscripted talk show, so long as she boosted ratings.
Smallpox wiped out Native Americans in state that now has the highest rates of vaccination exemptions
It seems particularly and painfully ironic that the state with the highest rate of parents opting out of childhood vaccinations is Oregon. This is a major public health concern, because when there are fewer people receiving vaccinations, herd immunity is reduced, making it easier for a disease to spread.
Oregon currently has the highest rate of unvaccinated children in the nation, well above the national average of 1.2%.
As of 2013, Oregon schools had the highest rate of non-medical–meaning religious–immunization exemptions for kindergarten age children. An all time high of 6.4% were exempt. That same year the state also recorded the highest rates for pertussis (whooping cough) cases in the United States, for the past 50 years, according to the Centers for Disease Control and Prevention (CDC).
According to the newsletter called the Lund Report: “In 2013, rates also showed that 17 counties have now surpassed the common 6 percent threshold whereby herd immunity may be compromised for some vaccine-preventable diseases such as pertussis and measles. In 2012, 13 counties were above 6 percent.”
Now, flash back more than two centuries, when the scourge of smallpox was first recorded in the Northwest due to trade with Europeans. A smallpox epidemic, starting in the upper Missouri River country, swept through current day Oregon to the Pacific Ocean in 1781–82 with horrific effects. Another scourge of “fever and ague,” likely malaria, ravaged Oregon in 1830–31. Other diseases as tuberculosis, measles, and venereal infections also took a huge toll. Epidemics in fact took an estimated nine of 10 lives of the lower Columbia Indian population between 1830 and 1834.
A rest stop on the Columbia River Gorge provides historic background on the dessimation of Native residents in Oregon due to disease in the 1800s.
In 1834, Dr. John Townsend, in the area that would become the Oregon Territory, wrote of a mass extermination of Native residents, similar in scope to what one today only knows through zombie or science fiction films of recent years like World War Z and I am Legend.
Townsend wrote: “The Indians of the Columbia were once a numerous and powerful people; the shore of the river, for scores of miles, was lined with their villages; the council fire was frequently lighted, the pipe passed round, and the destinies of the nation deliberated upon . . . Now alas! where is he? –gone; —gathered to his fathers and to his happy hunting grounds; his place knows him no more. The spot where once stood the thickly peopled village, the smoke curling and wreathing above the closely packed lodges, the lively children playing in the front, and their indolent parents lounging on their mats, is now only indicated by a heap of undistinguishable ruins. The depopulation here has been truly fearful. A gentleman told me, that only four years ago, as he wandered near what had formerly been a thickly peopled village, he counted no less than sixteen dead, men and women, lying unburied and festering in the sun in front of their habitations. Within the houses all were sick; not one had escaped the contagion; upwards of a hundred individuals, men, women, and children, were writhing in agony on the floors of the houses, with no one to render them any assistance. Some were in the dying struggle, and clenching with the convulsive grasp of death their disease-worn companions, shrieked and howled in the last sharp agony.”
An image shows the young then-U.S. officer Ulysses S. Grant, during his tour of duty on the Pacific Coast, where he saw the devastation of smallpox firsthand.
While stationed in Fort Vancouver on the banks of the Columbia River in 1852 and 1853, future Union General and President Ulysses S. Grant recorded similar devastation: “The Indians, along the lower Columbia as far as the Cascades and on the lower Willamette, died off very fast during the year I spent in that section; for besides acquiring the vices of the white people they had acquired also their diseases. The measles and the small-pox were both amazingly fatal. … During my year on the Columbia River, the smallpox exterminated one small remnant of a band of Indians entirely, and reduced others materially. I do not think there was a case of recovery among them, until the doctor with the Hudson Bay Company took the matter in hand and established a hospital. Nearly every case he treated recovered. I never, myself, saw the treatment described in the preceding paragraph, but have heard it described by persons who have witnessed it. The decimation among the Indians I knew of personally, and the hospital, established for their benefit, was a Hudson’s Bay building not a stone’s throw from my own quarters.”
(For those interested in this topic, they may wish to buy, download, or borrow a study of smallpox’s impact on Native North Americans called Rotting Face: Smallpox and the American Indian. One reviewer wrote that smallpox “claimed more lives from the Northern Plains tribes in one year than all the military expeditions ever sent against American Indians.”)
Where is the statue or monument pointing out this critical event in Oregon’s history?
Yet, I could find no record of any statue or memorial in Oregon today that notes this historic tragedy, which depopulated a region and left it wide open for white settlers to inhabit in the mid-1800s. Perhaps if such physical reminders were present, and educational programs to accompany them, there might be a more lively debate in Oregon. But as of now, it is state celebrated for its vaccination deniers and for denying the benefits of community water fluoridation for residents of its major urban center, Portland, for a fourth time since the 1950s.
Maybe a statue honoring ghost villages, dead tribes, and forgotten cultures on the banks of scenic Multnomah River in downtown Portland, could kick off with a special celebrity ceremony. The organizers could host a live broadcast of The View with Jenny McCarthy, in a revealing dress, describing why the state’s residents should keep their children from getting vaccinated from diseases such as pertussis.
I would be sure this event included representatives of the remaining tribal groups who managed to survive the wholesale disease-driven extermination of their brethren not many decades ago, many due to illnesses now controlled through childhood immunizations. Now that would be an attention-grabbing event that might just propel the discussion in a new direction.
Seattle traffic is among the worst in the nation, and it can be downright deadly, according to those who track road-related fatalities.
Every day that I drive to work, I am literally putting my life on the line. I commute roughly 80 miles daily, round trip, from Seattle to Tacoma, navigating one of the most harrowing urban traffic corridors in the Untied States, on Interstate 5 and two state highways. (My story why I am commuting this way will be for another day, but there are good reasons.)
Routinely, erratic drivers dangerously pass me, putting our lives at risk, in order to gain a few extra minutes by speeding. I have seen many accidents, some fatal, on this route over the years, and I am glad that I have my will and living will in proper order in case a truck jack-knifes near me in the rain—and yes I’ve seen that happen twice before on the freeway system around Seattle.
How deadly are roads in the Puget Sound–take a look at the roadkill on this data map showing types of mortality by form of transportation for 2001-2009.
Judging by this map, we get a fair share of road kill in the metro area I call home.
The Centers for Disease Control and Prevention (CDC) put the number of road deaths annually in my home state at nearly 500 (2009). Nationally, in 2012, the United States reported that 34,080 people died in motor vehicle traffic crashes in 2012, a 5.3% jump over 2011. This ranks as 10th leading cause of death in the United States, if one pulls this form of death from all accidental deaths, in which it is grouped by the CDC epidemiologists.
So by all counts, getting in one’s car (or on one’s bike or in a bus or other form of transportation) and hitting the road can be deadly business in my country, especially given the proliferation of mobile-device users and drunk drivers.
In 2011, cell phone use in the good ole’ U.S.A. was a contributing factor in more than 3,300 deaths and for the previous year, in 387,000 motor vehicle injuries. These are very sobering numbers, and I actually expected there would be more given that I have seen far too many texters during peak travel times in vehicles moving 70 mph. Normally I move over a lane or lay on my horn to snap them out of it.
But this is nothing compared to the perils that passengers and drivers experience globally. According to the World Health Organization (WHO), road accidents claimed 1.2 million lives globally in 2011, ranking as the No. 10 cause of death, on a list that has some pretty nasty company, including respiratory infections (3.5 million), tuberculosis (1.3 million), and the big killer of children ages 0-5 years, diarrhea (2.5 million).
A typical story that one sees with mind-numbing frequency overseas are bus collisions with motorcycles and motor scooters. This November 2012 story, 19-yr-olds crushed to death by bus, notes two aspiring young men were run over by an errant bus driver and dragged 40 feet in Chandigarh, India; the driver then fled the scene. Both of the men’s heads were crushed by the bus’s wheels.
I saw no less than three similar road maulings on the island of Java in 2009, when I visited Indonesia. That island, one of the most densely populated locations in the world, is overwhelmed with low-income and middle-income residents on scooters competing for space with trucks and army of loosely and unregulated van taxis and buses.
Indonesians who use these highly efficient and inexpensive 100-125cc motor scooters are frequently killed on the island nation’s infamously unsafe and crowded roads.
Road accidents alone in Indonesia account for more than 48,000 deaths annually, the 9th leading cause of death in the world’s largest Muslim nation.
The United States Department of State offers this stern warning to would-be American visitors to Indonesia–a country I really loved by the way: “Air, ferry, and road accidents resulting in fatalities, injuries, and significant damage are common. … While all forms of transportation are ostensibly regulated in Indonesia, oversight is spotty, equipment tends to be less well maintained than that operated in the United States, amenities do not typically meet Western standards, and rescue/emergency response is notably lacking.”
During my two-week visit in 2009 to the island nation, I rode about a dozen different buses and equally as many microbuses, not to mention the country’s crash-prone domestic air carriers once, their local train service (also unsafe at times), and the far less safe inter-island ferry services. I saw about a half dozen crashes from my bus window, most fatal and usually with motor cycle riders as victims, and from my hotel room I heard one multi-vehicle crash in the middle of the night that clearly claimed many lives. I learned the next day it was between a bus and truck. The bus was totaled.
Roads can really kill you overseas, and so can planes, boats, and trains too
Buses like these are cheap in Indonesia, but your life can be as some locals would say, insha-Allah, or at the mercy of God.
The writer Carl Hoffman, author of the book The Lunatic Express: Discovering the World… via Its Most Dangerous Buses, Boats, Trains, and Planes, documents the horrendous conditions of ferries, public transportation, trains, planes, and other forms of transport. The book’s online promotion notes that it offers a “harrowing and insightful look at the world as it is, a planet full of hundreds of millions of people, mostly poor, on the move and seeking their fortunes.”
Anyone who has travelled in developing or “middle-income” countries (like, say, Chile or Turkey) knows their life is literally in the hands of drivers who may have no proper training, in busses with no proper maintenance or even reliable brakes. Worse, the drivers of buses and microbuses in countries from Uganda to India to Mexico may trust their fate to Allah, Saint Christopher, the Virgin Mary, or Krishna. Those who have travelled in such places know this to be true, by the many religious deities dangling at the front of public transportation by the drivers’ seats.
Worse, the drivers will often play chicken with their competitors by speeding into oncoming traffic at high speeds while passing other vehicles or simply to “have fun.” I swear I thought I would die on many occasions in: Mexico, Guatemala, Nepal, Peru, Uganda, Indonesia, Egypt, Turkey, Chile, Argentina, India, and other places that I’d rather forget just now.
When is an accident really an accident, or when it is linked to larger systems issues? This analysis is provided by Anne-Emmanuelle Birn in her description of the social determinants of health (SDOH).
Three separate times, after I lived through the near mishap, I swore I would never, ever take a bus again in a developing nation. Yet I threw caution to the wind, as I needed to get around, and I could not afford to get around any other way. Not seeing the country I was visiting was not an option.
Is it really “just an accident” or something more?
Anne-Emmanuelle Birn, international health professor at the University of Toronto, and co-author of the widely used global health tome called Textbook of International Health, points out the deeper connections that road-related deaths have to poverty and social inequity in undeveloped and middle-income countries. Birn writes that road traffic accidents are the second-leading cause of death for children between 5 and 14 years of age globally, and that poor and working classes are disproportionately affected in most countries. In high- income countries, most of those killed are drivers and passengers, whereas in low- and middle-income countries pedestrians, cyclists, and public transport passengers make up nine out of every 10 road-related deaths.
In Haiti, for instance, the word for local transport is molue (“moving morgue”) and in southern Nigeria locals say danfo (“flying coffins”).
Duncan Green, an Oxfam policy adviser and development blogger, recently wrote an article asking when road traffic injuries would finally be recognized as a priority by the international development community.
In fact a major report released in June 2013 by the Overseas Development Institute, the United Kingdom’s leading development think tank, notes that transportation is not recognized as a human right like access to water, yet it still is a fundamental factor for many to achieve basic human rights. Well-run transportation systems, for people and for goods and services, promote benefits, while unsafe and weak transportation systems harm the most vulnerable citizens.
Given the debate emerging now for future sustainable development post-2015, the deadline set for the Millennium Development Goals, road safety may finally find a way into the broader public health, development, and environment agenda, as a way to tackle this clearly documented major global killer. Perhaps the threat may finally be treated as the international epidemic that is is, globally or closer to home in the United Sates. For me, this includes the roads in the Puget Sound where I spend more than two hours daily to and from my public health job.
News stories continue to highlight the growth of human trafficking in the United States, Europe, and especially Asia. One estimate puts the number of persons in captivity, either for forced bondage or sex trafficking and prostitution, at 12 million to 27 million. An increasing number of victims are young girls 18 and younger, who become infected with sexually transmitted diseases such as HIV/AIDs.
Slavery seems to bring out the worst of humanity, and perhaps is a manifestation of our inglorious inhumanity. Sadly it is, well, about as American as the U.S. Constitution that not only enshrined it, but gave Southern states extra voting power–the notorious 3/5ths clause–for its slaves in the census allotment of Congressional seats.
I still remember when I visited the Philippines in 2003. Male and female pimps repeatedly accosted me within seconds of exiting taxis in front of my hotels in Cebu City and Manila, where I was working on a photo-documentary project. I was sure their workers were sex slaves. When I told them to go away, they mocked me and even offered me young children. It was sobering to realize that I represented a market, a lucrative market, that eagerly comes to countries like the Philippines, Thailand, Cambodia, and Laos to exploit women, even young boys and girls. Though aware of the problem, and having seen evidence of its freewheeling nature in Asia, the unrelenting media coverage of sex slavery has become overwhelming.
Time Magazine reported on slavery in Embassy Row in the nation’s capital three years ago, but it can happen anywhere in the United States.
In April 2013, European Union Home Affairs Commissioner Cecilia Malmström lamented: “It is difficult to imagine that in our free and democratic EU countries tens of thousands of human beings can be deprived of their liberty and exploited, traded as commodities for profit.” The United Nations estimates human trafficking nets $32 billion annually—a major transnational business. The United States fares no better. There are slaves being trafficked and sold in my home city of Seattle right now. A local KIRO News story recently reported: “Child sex trafficking – as easy in Seattle as ordering a pizza.”
Visiting Osawatomie, and its place in U.S. history
So slavery was on my mind when I drove across the country in late May from St. Louis to Seattle. I wanted to take a road less traveled and see some out of the way places, including in Kansas. Most of my friends practically laughed at me when I described sight-seeing there. So, I pulled out my atlas and found Osawatomie on the map, about an hour southwest of Kansas City, along state Highway 169
Specifically, it is where America’s most famous abolitionist and violent revolutionary, John Brown (1800-1859), fought pro-slavery forces to prevent the then Kansas Territory from becoming a slave state. All told 30-45 free state defenders, known as Jayhawkers (the University of Kansas’ namesake) fought nearly 250 proslavery militia along the banks of the Marais de Cygnes River on Aug. 30, 1856. Brown’s son Frederick and others died. Many say the war actually began in this small Kansas town that pro-slavers burnt to the ground during the attack.
Entrance to John Brown Memorial Park in Osawatomie, Kan.
In May of that year, Missouri ruffians, numbering 800, had sacked Lawrence, Kan., and burned a hotel, killing one abolitionist. Their strategic goal was to keep an entire race of persons in human bondage and treated as nothing more than property, and expand the inhumane practice and trade into territories recently “ethnically cleansed” of its Indian population by the U.S. Army, based at Ft. Leavenworth.
On May 24 and 25, 1856, at the so-called Pottawatomie Massacre, Brown responded in kind, by murdering five pro-slavery settlers with a sword. The mass murder by Brown and his sons was inspired by Brown’s deep Christian faith that he had been called to undertake a divine mission to end slavery and contest its brutality and those of its violent supporters with force.
The repeated and well-publicized examples of slavery’s inhumanity in the United States enraged Brown to the point where he dedicated his life to crushing it and freeing the slaves. (Unlike most of his day, Brown also believed in the equality of races, including Indians, and of the sexes.)
Just two years earlier in 1854, a divided Congress passed the Kansas-Nebraska Act, ending the fragile 24-year-old Missouri Compromise allowing a balance of pro-slave and free states to join the Union. With the 1854 act, settlers themselves would determine if that “peculiar institution” of slavery, which held in bondage an estimated 4 million persons, or 13% of all residents in the young country, would be allowed. Pro-slavery voters won, but the constitution was disavowed, the bogus legislature tossed out, and Kansas entered a free state in 1861.
One historic political outcome from the four years of fighting in the territory was the rise of a young Illinois politician of the nascent Republican Party, who noted in his political speeches, “Look at the magnitude of this subject! … about one-sixth of the whole population of the United States are slaves!” Abraham Lincoln emerged from the turbulence of the era as the standard bearer of his party in the divisive 1860 election that set in motion the war to address what Lincoln accurately noted was the “the all absorbing topic of the day.”
As for Brown after Osawatomie, he travelled in and out of Kansas the next two years of violence before returning East to plan his failed Oct. 16, 1859, raid on the federal armory in Harper’s Ferry, Va. The raid, with 21 men to trigger a Southern slave uprising, failed miserably.
A statue of the abolitionist and revolutionary John Brown stands guard at a park with his namesake in Osawatomie, Kan.
Brown was captured, tried in Charlestown, Va., and sentenced to hang to death on Dec. 2, 1859. During his trial he told the court, “Now, if it be deemed necessary that I should forfeit my life for the furtherance of the ends of justice, and mingle my blood further with the blood of my children, and with the blood of millions in this slave country whose rights are disregarded by wicked, cruel, and unjust enactments, I submit: so let it be done.”
Southern politicians were terrified by Brown’s decisive and violent insurrection against the U.S. government and their “cherished traditions.” Their paranoia of either a slave uprising or further such “meddling” precipitated their rebellion against the union.
All of that history seemed overblown and forgotten in modern-day Osawatomie (pop. 4,447). The memorial to Brown and the battle is the John Brown Museum State Historical site. It includes a cabin of a local minister and his wife used as an Underground Railroad station. The cabin survived the battle. The park features a bronze statue of Brown and historic battle markers. It looked a little shabby and unappreciated, like any small-town park without money for upkeep, except it has happened to have two presidential visitors who delivered policy speeches, by Teddy Roosevelt in 1910 and Barack Obama in 2011.
Hollywood, Slavery, and the Battle for Kansas
For many of us, however, our perception of slavery is shaped by popular culture. One of two most recent Hollywood treatments of the subject was the scholarly costume epic Lincoln, by Stephen Spielberg. The film did not hide the brutality of slavery; in fact, the film opens with a vicious hand-to-hand battle pitting likely former slave Union soldiers locked in deadly embrace with their white Confederate adversaries. The film is basically a procedural drama how Lincoln’s administration passed the 13th Amendment to the Constitution, to end slavery “forever” in United States, while the nation’s most violent war rages outside of Washington.
The more controversial rendering of slavery is the 2012 Quentin Tarantino blood and gore pre-Civil War spectacle, Django Unchained. This shoot-‘em up racks up a huge body count in a gratuitously violent revenge fantasy that follows the actions of a former slave, Django, played by Jamie Foxx. He kills perhaps nearly two dozen Southerners, blows up plantation mansions, and frees his true love. Unlike Lincoln, this film was heatedly debated. One review noted, “No single Hollywood film in the last decade has sparked the kind of controversy and wide-ranging response as Quentin Tarantino’s latest.”
The film triggered unrest not because of its brutal violence (nothing new for Hollywood splatter fests), but because of its rival view of history. “The most important thing about Django Unchained is that it’s a reaction against, or corrective of, movies like Birth of a Nation and Gone with the Wind. At every turn, it subverts or inverts the racist tropes that have defined Hollywood’s–and our culture’s–treatment of slavery, the Civil War, and Reconstruction,” according to Jamelle Bouie.
I have black friends who had a distinctly more positive personal reaction to the violent tale than did my white counterparts. While the film’s violence seems designed only thrill audiences, the violence of slavery and of efforts to expand it by pro-slavery bushwhackers in Kansas before and during the Civil War was every bit if not more cruel, if historical records are accurate. Reality actually trumps anything Tarantino could dream up.
The magazine Harper’s printed an illustration of the 1863 raid by Southern bushwhackers of Lawrence, Kan, which killed 180 people.
According to one account, a bushwhackers’ raid during the Civil War on Lawrence, Kan., is considered one of the worst cases of mass murder by the pro-Slavery forces.
On Aug. 21, 1863, 450 pro-Confederates Led by Bill Quantrill staged an early-warning raid and mostly showed no mercy, slaughtering about 180 men and boys as young as 14. Most of the victims were unarmed and still in their beds when the killing began. Another famous bushwhacker in the region, a psychopath named “Bloody” Bill Anderson, reportedly scalped victims before he was tracked and killed, and then beheaded as an example.
The official Hollywood rendering of “bleeding Kansas” and John Brown’s efforts to end slavery remains Michael Curtiz’s unsavory pro-slavery 1940 Western called the Sante Fe Trail (you can see the whole film here). The movie stars Errol Flynn as future Confederate General Jeb Stuart, then-actor Ronald Reagan as future Indian-killing General George Custer, and Olivia de Havilland as their mutual romantic interest. The film renders a staggering historic whitewash of not only slavery and pre-Civil War America, but of John Brown’s actions in Kansas to contest the bushwhackers during the mid- to late 1850s.
Brown is portrayed by Raymond Massey as a bug-eyed, villainous psychopath bent on murder and revolution to end slavery, while Southern gentlemen like Flynn’s Stuart are true Americans who claim the South can work out slavery on their own terms. There is no portrayal of slavery’s base cruelty, only abolitionist violence in Kansas and at Harper’s Ferry.
Raymond Massey portraying John Brown on his hanging day on Dec. 2, 1859–an event that sped the nation faster to Civil War.
In an even more bizarre twist, future Confederate President Jefferson Davis is rendered as moral voice of wisdom, telling the graduating cadets: “”You men have but one duty alone, America.” This was the same Davis who owned slaves and dedicated himself to ensuring slavery’s survival as head of the pro-slave states doing everything they could to break away from that country.
The pro-slavery 1940 film Sante Fe Trail featured escaped slaves as subservient, pro-slavery fools who desired to return to plantation life rather than chase freedom with John Brown.
The only “black folk” seen in this disingenuous Dixie-cratic rendering of reality are powerless, witless slaves who cannot think for themselves. After a firefight that sent Brown fleeing, a husband and wife slave couple from Texas caught up in Brown’s violence reveal themselves to Stuart as misguided lovers of the white slaveholding class: “Well, old John Brown said he gonna give us freedom but, shuckin’, if this here Kansas is freedom then I ain’t got no use for it, no sir,” drawled the wife. Her husband added, “Me neither. I just want to get back home to Texas and set till kingdom come.” I suppose that means he’d get a good whipping if he fessed up for trying to win his freedom.
As one film commentator noted: “In the years before 1960 most portrayals of slavery in cinema were like it was in Gone with the Wind and Jezebel. The slaves were happy and contented and too simple to live on their own. The Civil War was unnecessary and brought on by a handful of fanatics in the North.” The film’s final scenes show Brown before he is hung in 1859, followed by a happy kiss of the newlyweds, Flynn and de Havilland, all two years before the entire country entered its greatest conflagration that claimed more than half a million lives, finally “ending” slavery as a legal institution in the United States.
Former Klansman becomes part of Hollywood whitewash of Southern bushwhacking
The other noteworthy and historically inaccurate portrayal of Kansas-related bushwhacking violence is Clint Eastwood’s disturbing 1976 revisionist film The Outlaw Josey Wales. While supposedly based on a true Southern fighter, the film rewrites the script of historic events. Instead of violent Confederate bushwhackers who murdered indiscriminately, as they did in Lawrence, Southerners are portrayed as victims of murderous Jayhawkers and Union soldiers, who kill innocent women and slaughter surrendering prisoners, and hound Wales to Texas. The film was based on a novel, Gone to Texas, by Asa Carter, also author of a popular kid’s book called the Education of Little Tree.
At the time the film was made in 1976, it was unknown that Carter had reinvented himself. Instead of being a Cherokee Indian as he claimed, Carter was in fact a former Alabama Klansman, avowed racist, and speechwriter for Alabama’s segregationist Governor George Wallace. The books served as a clever reinvention for a man preaching against “government intrusion,” as Carter did for Wallace with racist hate language. Even his supposed Cherokee words were fiction. As for Josey Wales, the film helped to reinforce Southern stereotypes of Northern aggression and Southern innocence (despite its holding 4 million in captivity), while boosting Eastwood’s maverick filmmaking career.
In 2013, in an era when slavery seems to be as thriving an enterprise globally as it was in the antebellum South, perhaps it is time reexamine on the big screen the complex events in Kansas and Virginia and that fanatical revolutionary who committed his life to ending the institution forever. I just do not want the filmmaker to be Eastwood, Tarantino, or even Spielberg, nor a vampire camp production. Time to let someone else tell a tale that still needs to be told. Love or hate him, Brown was right about slavery’s stain on the nation. Brown’s enemies “could kill him,” wrote freed slave and fellow abolitionist Frederick Douglass, “but they could not answer him.”
On May 17, 2013, I participated with other employees in my public health department working at Project Homeless Connect. This is, at present, a quarterly endeavor to provide a range of medical and social services to the estimated 2,000 homeless individuals of Pierce County, Washington.
However, the people who line up as early as 7 a.m. for a range of needed services are not entirely the homeless. Many have jobs, but lack health and dental insurance. They basically are coming for primary or even emergency care that they cannot access elsewhere.
The Washington State Department of Social and Health Services was one of many organizations participating in Project Homeless Connect, held on May 17, 2013 at Calvary Community Church, in Sumner, Wash.
Project Homeless Connect, in its communications for its volunteer-run event, said it offered the following:
Medical and urgent care
Urgent dental care
Mental health services
Social service referrals
Vision/glasses
Haircuts
Child/adult immunizations
Veterinary care
Legal and financial advice
Housing, shelter, employment and education information
Tobacco cessation
Homeless assistance
Veterans services
Chemical dependence and assessment
This was no small effort. Months of planning went into pulling off this disaster-relief style engagement that is more associated with hurricanes and tornadoes than with meeting the basic needs of Pierce County, the second most populous (pop. 812,000) in Washington State.
Large, converted vans/trucks lined up providing veterinary services, dental care, and other interventions. Yet, oddly, there was no media present to put the story on the 5 p.m. news or in the daily newspaper the following day. (I checked but found nothing doing Google searches.) Why? Everyone who was homeless in Pierce and most social service and medical service providers likely was aware the event was taking place, for months in advance.
I did see not any elected officials (they may have come, and they may even have volunteered). All of this took place in a county whose hospitals are making profits of $1,000 per patient visit more than the state average and in a county where nonprofit hospitals are earning up to and more than $500 million in profits.
I saw all kinds of people—young, old, white, black, Asian, Latino, Pacific Islander, disabled, able-bodied, veterans, you name it. Volunteers came in all stripes as well. There were military personnel, dental assistant students from Pierce County community colleges (Bates and Pierce ), trained medical providers, church volunteers, hair stylists, and more. The list goes on. What struck me the most was how polite and appreciative the attendees were. Many drove or were driven from remote parts of the county to this somewhat semi-rural area in Pierce, southeast of Tacoma.
One of the providers, Medical Teams International, had one of its full-service converted mobile home vans providing dental care.
Medical Teams International brought one its converted mobile home vans to Project Homeless Connect on May 17, 2013, in Sumner, Wash.
That program boasts a fleet of 11 mobile dental clinics in Oregon, Washington, and Minnesota that use 38-foot converted motor homes. Each clinic contains has two full medical stations and all necessary equipment, instruments, and supplies. The organization claims it has helped more than 200,000 adults and children with its mobile medical program since 1989.
Medical Teams International defines itself as a christian global health organization “demonstrating the love of Christ to people affected by disaster, conflict, and poverty.” The group works globally, including in Africa, South America, Asia, and North America.
Yet, it was in Pierce, addressing what clearly that organization perceived as akin to disaster and conflict.
All of this I find remarkable. Less than five miles from this revolving quarterly circus of human need there was a major shopping center, South Hill Mall, with about every major electronic gadget and consumer good on the market. Truck and car lots were also close by, with products selling from $25,000 and up. The disconnect to me was palpable, particularly the same week the Republican-led U.S. House of Representatives passed its 37th legislative measure to repeal or defund the market-driven health care reform known to its detractors as “Obamacare.”
I recall what one of my University of Washington School of Public Health colleagues—the one I respected more than nearly all others—told me when we talked about our peers who had worked or would work in public health in Africa or in developing nations. My friend asked somewhat ironically, why don’t they work at home. We have plenty of problems here. Given what I saw at Project Homeless Connect in Pierce County in mid-May 2013, I could not agree more.
Milla Jovovich in her role as Joan of Arc in the film The Messenger: the Story of Joan of Arc.
Recently, I watched a movie about the life of Joan of Arc (Jeanne d’Arc) called The Messenger, the Story of Joan of Arc by French director Luc Besson and starring Milla Jovovich. Though the movie got tepid reviews, I was mesmerized by it.
The period epic faithfully re-tells many key moments in the short life of the world-renown young French leader, including her actual words that were recorded in detailed written accounts. I found the movie intoxicating because of Jovivich’s exuberance as Joan, inspiring her countrymen to arms to free their nation, ensuring the crowning of the Dauphin Prince in the Reims Cathedral as King, and following in her view the will of God.
Few other single individuals had such an impact on world history as this illiterate peasant girl, who rose to prominence in a violent male world and became one of history’s greatest and most inspirational figures—and a saint for Catholic believers. In fact, at the mess hall at West Point, a mural depicting history’s greatest military leaders includes a rendition of Joan, with her holding a sword and in full body armor.
In fact no single historic figure from Europe during the 100 Years War between France and England remains as famous today as Joan. By the age of 17, she unswervingly acted on voices in her head telling her to drive the English from France and crown Charles VII as King of France. This came at France’s weakest moment in its history, with the English and Burgundians in control of half the country.
Yet, this virtual unknown girl never waivered. She gained access to the French court in the spring of 1429 in Chinon, France. She withstood questions from learned and suspicious church officials and a virginity test. She arrived in the besieged city of Orleans in April that year, bearing a standard and ready for action.
In defiance of cautious male commanders, she singlehandedly helped lead the French to defeat the attacking English, suffering several nearly fatal injuries. Her foes called her a witch and remained fearful of her talismanic powers. She brought together violent, power hungry men, like the Count of Dunois and the Duke of Alencon, around a common cause to the point they even would stop swearing and offered blind loyalty to her. Most importantly, she restored confidence of the French people around a common goal. Soon, all of Europe was talking about the Maid of Orleans and her battlefield exploits.
Joan of Arc being burned at the stake after being tried by the English and church leaders in 1431. She was only 19 years old.
By July that year, Charles VII was crowned king. Yet within a year, the young peasant who worked miracles was captured and ransomed to the English, tried as a heretic, and burned at the stake in Rouen on May 27, 1431, for having worn men’s clothes, no less.
Five centuries after her murder, she was pronounced a saint by the Catholic Church for the miracles that are linked to her remarkable accomplishments. While she did promote violence, she always offered her opponents opportunities for peaceful alternatives, and she reportedly showed great kindness to those captured.
So why should anyone in public health care about Joan of Arc?
As a student of history, I found many elements of her remarkable story relevant for my reality. Instead of beleaguered 15th century France, I find myself in the reality of the beleaguered U.S. public health system.
Religion you say? That has nothing to do with healthcare and public health, right? Well, that ignores the fact that religion has everything to do with healthcare and public health. For example:
Well, an illiterate peasant girl can teach nothing of value to doctors, PhDs, and other well-educated professionals who run our nation’s public health system, right?
I recently read an article highlighting leadership and public health. Some of the attributes associated with leadership include: serving, complex thinking, being a change agent, self-empowerment to empower others, risking failure, creating a future one envisions, and being confident in one’s beliefs and then living the change one wants. I am actually hard-pressed to find examples of such traits in leaders in my field who are resonating widely with the American public. Joan of Arc consistently showed all of these leadership traits, from risking her life on the field, to being a catalyst, to having supreme confidence in her vision.
Former U.S. Surgeon General and “Public Health Hero” Dr. David Satcher.
In the United States, there are always “unsung hero” awards for people who no one outside of the particular field giving the award have heard of, or even care about, it seems. While these may help sustain the field of providers, they likely do little to inspire the public.
The University of California Berkeley in February held its annual event for “public health heroes,” awarding its 2013 prize to former U.S. Surgeon General Dr. David Satcher. However, I doubt few Americans know who Dr. Satcher is, what he accomplished, and why such facts matter to the nation’s crisis of promoting public health in the 21st century.
This is not to belittle Dr. Satcher’s many accomplishments, such as his calling attention to the oral health epidemic in the United States. (Oral health experts have been talking about his report for more than a decade because he and it were spot on.)
Public health, teetering like France before the arrival of Joan of Arc?
Of course medieval France has nothing in common with the reality of modern America and its healthcare system, right? But if you take the view of that history can teach open-minded students of the present many valuable lessons, regardless of their field, one might find parallels.
France at Joan’s time was on the verge of collapse, lacking strong leadership and a vision to restore hope and unity. Joan arrived completely confident in her vision and religious mission, and she never wasted a day. She famously said, “Better today than tomorrow, better tomorrow than the day after.” She also is remembered by her words, “go forth boldly.” Such words and such inspiration are lacking in the U.S. public health system, to me at least.
For those working in the field of public health, one is constantly exposed to the reality of budget cuts that continue to hack away at programs that do everything to promote chronic disease interventions to immunizations. Between 2008 and 2010 alone, in the aftermath of the Great Recession, more than half of all local public health departments had cut core funding and shed 23,000 jobs, as well as cut programs, mainly due to falling tax revenues that hammered local and state funding.
Things continue to spiral downward as the recession’s effects linger, and mandatory across the board federal budget cuts known as the sequester will soon impact every local public health department in the country and national agencies who help fund local efforts. The Public Health Institute warned that sequester related cuts will be “devastating to the public’s health.” Such cuts, the institute says, “will cost jobs and resources in the short run, and the long-term costs—in money and lives—will be borne by families and communities for years to come.”
Crises also prevent departments from looking to innovation as they focus on life support and triage. Morale suffers, which impacts service and core functions. Leadership, perhaps what little that may exist in this beleaguered environment, is lacking. Public health managers struggle to connect with the public about what public health is and why it matters.
They fail to show that the U.S. health system’s treatment, not prevention, focus is largely unsustainable for the population’s health and the economy. In 2009, U.S. public health spending (at all governmental levels) amounted to $76.2 billion – only 3% of the nation’s overall healthcare outlays of $2.5 trillion. Yet, chronic diseases, which public health efforts can address, make up three quarters of all health care costs.
Public health spending, as measured as billions of dollars, versus all other healthcare spending in the United States and spending on chronic diseases and all other healthcare costs.
Reform does happen, and it can be bold when breakthroughs capture the public’s and globe’s attention.
HIV/AIDS assistance, which is now at the heart of a larger global public health agenda, was launched in the late 1990s when activists outside of the medical and public health establishment demanded that antiretroviral drugs, or ARVs, be made available to many of the world’s poorest and most afflicted nations, most in Africa, to reduce the spread of the virus inside the bodies of infected people and make it possible for them to live long lives.
It was not reformers inside “the system,” it was radicals outside “the system,” who offered a clear vision and the groundswell for change that the establishment eventually fully embraced.
As someone who works inside “the bureaucracy,” however, I am ever mindful of how the great Joan of Arc was ultimately marginalized, tortured, and burned alive at the stake for her completely unorthodox ways that challenged nearly all in authority in her day. The English did not trigger her downfall, it was palace politics and sexism, and likely fear of her power.
One of many Joan of Arc statues in France honoring one of the French nation’s greatest heroes.
The lessons are telling today. You can work miracles, but the machinations of any bureaucratic system can be deadlier than slings and arrows of a battlefield of your sworn enemies. You could transpose the palace intrigues of 15th century French and English courts to any bureaucracy today and it would be a near perfect fit, really. Would any bureaucratic leader trust an uneducated, poor, unconnected interloper to provide a vision for change for the failing health and public health system, such as the one facing the United States in 2013?
Sure, such a thought is laughable, but it happened, and can happen again. It may even be needed if things continue on the present course.
In the end, no one remembers the bishops who tried and convicted Joan or the weak king she helped to bring to power, or in fact any of the kings of her day. Likewise, no one remembers or cares about bureaucrats in the end. Why? Quite simply they are not visionaries.
It is Joan who has statues in her honor, countless biographies recounting her legend, and many movies and documentaries exploring her incredible exploits.