Some might say TV host Bill Maher is so political that he cannot be trusted. I disagree.
On March 8, on his TV show, Maher delivered a very provocative commentary that everyone in the field of health promotion, public health, and public policy should watch. Maher rightly asked, “Since when in America did everything have to be so political?” It was a smart piece of punditry, because he correctly showed how efforts to promote public health, nutrition, and healthy eating had become as politicized as the debate over regulating the proliferation of firearms.
Showing pictures of First Lady Michelle Obama, a champion of a national nutrition and exercise campaign called Let’s Move, Maher opined, “If seeing this nice lady on TV saying she likes the movies, or nutrition, or exercise fills you with rage, get help.”
Maher further correctly noted, “Big portions, conservative; knowing where your food came from, liberal.” In short, Maher said what few in the public health profession are saying or have the courage to say—that a deep schism exists in the public space that taints and will continue to taint all efforts to tackle some of this country’s biggest health problems.
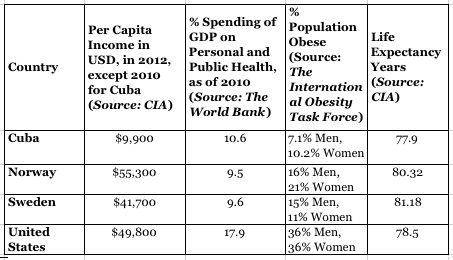
These include the obesity epidemic and the threat posed to our healthcare system and our national health by chronic disease.
Ever a political lightning rod who is ready to fan conservative flames, former half-term Alaska Gov. Sarah Palin used her speaking appearance at the 40th annual Conservative Political Action Committee (CPAC) conference on March 16, to lambaste New York City Mayor Michael Bloomberg’s efforts to tackle obesity by limiting the size of sugary-sweetened beverages. Bloomberg’s New York City law to limit the serving size of such drinks to just 16 ounces was overturned by a New York State Judge on March 11.
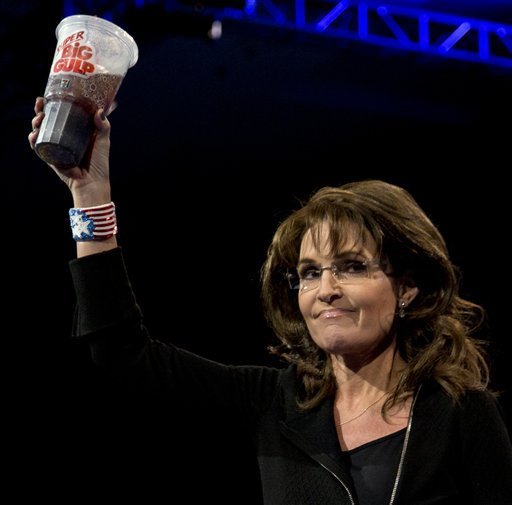
Completely ignoring the obesity crisis that is afflicting her own former state and the country, where two-thirds of all residents are obese or overweight, Palin slurped soda from a 7-11 Big Gulp. The theatrics, all perfectly inline with Palin’s anti-government theology, again proved Maher’s point about the politicization of even micro efforts by some local elected officials to address the public health threats facing the country. (Side note, Palin briefly was governor when I lived in Alaska, and I saw her at health promotion events like community runs–an action that she likely would brand as “liberal” today.)
Whenever I would engage Puget Sound area public health officials during my two years of study at the University of Washington School of Public Health (2010-’12), I always asked, how can you prevent the public perception that efforts to promote healthy activity and nutrition are not perceived by conservative voters and Republican elected officials as part of a liberal, activist agenda. I never got a good answer, mainly because I do not believe those officials had an answer. I did not draw any great wisdom from my faculty or UW SPH peers either.
Some wonkish types have tried to investigate this issue in “philosophical terms,” along traditional axes of egalitarianism/choice minded conservatism against regulation-minded “big government” liberalism. One 2005 article on responsibility in health care choices argued, “Holding individuals accountable for their choices in the context of health care is, however, controversial.” There may be some truth to this, but I discount the “core political values” explanation as a way of understanding the politicization of public health initiatives.
Perhaps the biggest fight in the U.S. political system today is over tax policy and the future of major social/medical programs—Social Security, Medicare, Medicaid—that provide the true underpinning to the public wellness of our country. This is, at its core, is vicious political battle that will shape the public health of the country unlike any action taken by any regulatory or health agency of the U.S. government.
Regulation to promote health has been at the heart of the public health enterprise ever since the field emerged as a profession in the United States in the late 1800s. According to the Centers for Disease Control and Prevention, many of the most successful public health achievements of the 20th century (food safety, motor vehicle safety, identifying tobacco as a health hazard, etc.) were “upstream” interventions that, by definition, were regulatory in nature and thus purely political.
However, public health, by being a public enterprise, is by definition a creature of the political process, and thus influenced through the power of the purse to curtail its authority and stymie its reach. Public health departments today, for instance, are managed by publicly accountable officials. A local public health department board of health, like King County’s, includes a broad range of elected officials and a few medical professionals.
The nation’s leading de facto public health official, the U.S. Surgeon General (Dr. Regina Benjamin), today remains a mostly toothless position that has little if no sway over the public policy debate concerning the nation’s public health, according to New York Times health blogger Mark Bittman. He writes, “… there is no official and identifiable spokesperson for the nation’s public health, and the obfuscation and confusion sown by Big Food, along with its outright lies and lobbying might, has created a situation in which no one in power will speak the truth: that our diet is making us sick, causing millions of premature deaths each year and driving health care costs through the roof.”
I personally believe that the position of Surgeon General remains that of a paper tiger because those who have power, members of Congress and the Executive Branch, do no wish to allow an advocate for public health to embarrass them with pesky things like facts and science that call for action.

The most effective Surgeon General in living memory who recently passed away in February, the late Dr. C. Everett Koop, proved unpredictable. Though a staunch conservative appointed by President Ronald Reagan, Dr. Koop staked out very controversial political positions on moral and medical grounds, in defiance of his boss, Reagan.
His notable actions still stand out today for their audacity to challenge powerful interests and their embrace of morality as a tactical advocacy tool:
- Koop’s office produced the plainly worded, 36-page “Surgeon General’s Report on Acquired Immune Deficiency Syndrome,” which clinically detailed HIV transmission, making clear it was not spread by casual contact and affirming that, “We are fighting a disease, not people.” Koop promoted sex education and condom use, enraging conservative critics.
- Koop also took on the all-powerful tobacco industry and lawmakers who received its many contributions with his pronouncements that smoking killed and should be banned. He famously called purveyors of cigarettes the “merchants of death.” (When is the last time anyone has heard a medical leader embrace such powerful language for a public health cause?)
Though Koop reportedly claimed morality never “clouded his judgment,” he remained an effective advocate on the bully pulpit by literally shaming those in power. “My whole career had been dedicated to prolonging lives,” he said, “especially the lives of people who were weak and powerless, the disenfranchised who needed an advocate: newborns who needed surgery, handicapped children, unborn children . . .people with AIDS.”
I keep waiting for someone, anyone besides billionaire Mayor Bloomberg, to enter the political discourse on behalf of public health and use straight language that cuts through the hype. The problem is, they cannot teach you leadership when you enter the fields of public health or politics. It is something you either are capable of, or simply lack. Right now, it is lacking.